Maxillary anterior guided orthotic
A Comprehensive Clinical and Scientific Review of the Maxillary Anterior Guided Orthotic (MAGO)
Executive Summary
This report provides a comprehensive clinical and scientific review of the Maxillary Anterior Guided Orthotic (MAGO), a specialized, removable dental appliance. The MAGO is primarily utilized as a non-invasive diagnostic and therapeutic tool for individuals suffering from temporomandibular disorders (TMD), bruxism, and associated craniocervical symptoms. Its fundamental principle is to deprogram the masticatory muscles and allow the mandibular condyles to seat in an orthopedically stable, physiologic position, thereby alleviating pain and dysfunction. This is achieved through an anterior guidance mechanism that disengages the posterior teeth, interrupting the neuromuscular patterns that perpetuate muscle hyperactivity and joint strain. A critical finding of this review is that the MAGO is not intended as a standalone cure but rather as an essential preliminary phase of treatment. Its primary function is diagnostic: to reveal the patient's true, unstrained jaw relationship. The successful stabilization of the jaw with a MAGO is the prerequisite for a definitive diagnosis and the subsequent, often irreversible, second phase of treatment, which may include occlusal equilibration, restorative dentistry, orthodontics, or orthognathic surgery. This positions the MAGO as a gateway to comprehensive occlusal reconstruction, a fact that has significant implications for patient education and informed consent. Furthermore, this report critically examines the recurring claim that MAGO therapy is the "only" scientifically proven splint therapy for TMD. This assertion is traced to a single 2015 retrospective cohort study on the Bioesthetic Maxillary Anterior-Guided Orthosis (BMAGO), a device with a specific philosophical underpinning. While the results of this study were positive, its observational design places it at a lower tier in the hierarchy of evidence compared to randomized controlled trials (RCTs) and systematic reviews. The broader scientific literature, including several meta-analyses on occlusal splints, presents a more equivocal and, in some cases, contradictory view on their long-term efficacy. In conclusion, the MAGO represents a valuable diagnostic modality within specific clinical philosophies, offering a reversible method to establish a stable foundation for complex dental treatment. However, its efficacy must be considered within the context of a comprehensive, multi-stage treatment plan. The discrepancy between marketing claims and the broader body of scientific evidence underscores the need for high-quality RCTs to definitively establish its specific benefits over other occlusal appliance designs and conservative therapies. Clinician expertise in diagnosis, meticulous appliance adjustment, and a deep understanding of occlusal principles are paramount to its safe and effective application.
I. Introduction to the Maxillary Anterior Guided Orthotic
The Maxillary Anterior Guided Orthotic (MAGO) is a specific type of intraoral occlusal appliance designed to address dysfunction within the masticatory system. Unlike generic night guards, which primarily serve a protective function, the MAGO is engineered with both diagnostic and therapeutic objectives. Its design and management are rooted in principles of gnathology and neuromuscular physiology, aiming to re-establish a harmonious relationship between the temporomandibular joints (TMJs), the masticatory musculature, and the dentition.
1.1 Defining the MAGO: Deconstruction and Synthesis
The name of the appliance provides a direct description of its design and intended function. The acronym MAGO stands for 1:
- Maxillary: The orthotic is fabricated for and fitted to the upper dental arch (the maxilla).
- Anterior: It utilizes the front teeth (the anteriors) to control mandibular movement.
- Guided: Its primary function is to guide the mandible into a specific, predetermined relationship with the cranium.
- Orthotic: It is an orthopedic device designed to support and stabilize the jaw joints, analogous to an orthotic used for other joints in the body, such as the knee.1
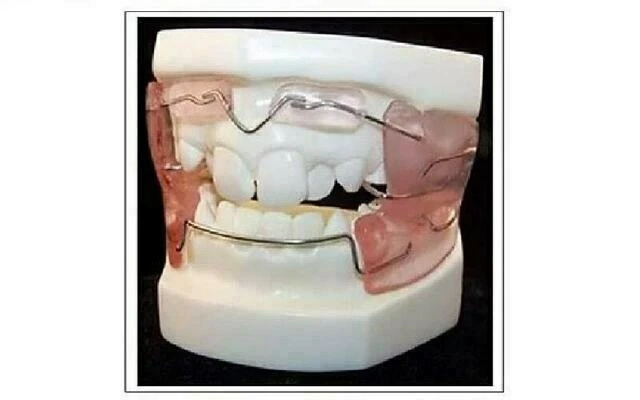
The MAGO is a custom-made, removable appliance, typically fabricated from a clear, hard acrylic resin.1 While some clinical descriptions specify that it is a device worn over the front teeth 2, the broader context of occlusal splint therapy, including its fabrication, suggests it is more accurately a full-coverage maxillary splint that incorporates a specialized anterior guidance ramp.8 This design provides orthopedic stability for the entire head and neck through the dental arches.1 A central tenet of MAGO therapy is its dual functionality. It is simultaneously a diagnostic tool and a therapeutic intervention.1 As a therapeutic device, it provides immediate relief from symptoms such as chronic jaw pain, headaches, and muscle fatigue.9 As a diagnostic tool—its more critical function—it is used to find the underlying cause of a patient's symptoms by revealing the true, unstrained position of the jaw.2 This dual-purpose nature is fundamental to understanding its role in a comprehensive treatment plan.
1.2 Core Principles and Therapeutic Goals
The foundational principle of MAGO therapy is the stabilization of the temporomandibular joints. The therapy operates on the premise that a patient's habitual bite, or maximum intercuspation, is often a position of accommodation to a malocclusion, forcing the masticatory muscles and jaw joints into a strained, pathological state.6 The MAGO is designed to interrupt this cycle. The primary therapeutic goals are: 1. Muscle Relaxation: By creating a smooth, idealized occlusal surface with specific anterior guidance, the MAGO eliminates disruptive tooth contacts that trigger muscle hyperactivity. This allows the powerful chewing muscles to release from a state of chronic tension and spasm.6 2. Joint Seating: Once the muscles are relaxed, the mandible is no longer held in a strained position. The MAGO guides the jaw, allowing the condyles (the "ball" of the jaw joint) to seat themselves into their most stable and physiologically sound position within the glenoid fossae (the "socket").1 This is often referred to as allowing the jaw joints to "go home".1 3. Symptom Resolution: Achieving a relaxed musculature and a stable joint position leads to a reduction in inflammation and the alleviation of a wide range of TMD symptoms, including headaches, migraines, ear pain, facial pain, and joint noises.3 4. Functional Improvement: With the system stabilized, patients typically experience improved jaw function, enabling more comfortable chewing, speaking, and swallowing.3 Ultimately, the MAGO is not viewed as a permanent solution but as a transitional device. Its success in relieving symptoms serves to validate that the patient's problems were indeed related to an unstable bite and joint position. This validation then forms the basis for a definitive diagnosis, which is the necessary precursor to long-term, corrective treatment.1
1.3 The MAGO and BMAGO Distinction: A Critical Clarification
A critical analysis of the available literature reveals a significant point of ambiguity concerning the evidence base for MAGO therapy. Many clinical proponents make the emphatic claim that MAGO therapy is the "ONLY" type of splint therapy that has been scientifically proven to be effective for treating TMD symptoms.7 This claim is consistently traced to a single cohort study published in 2015.15 However, a direct examination of this foundational study reveals that the device investigated was a Bioesthetic Maxillary Anterior-Guided Orthosis (BMAGO).16 The "Bioesthetic" prefix denotes a specific clinical philosophy that seeks to emulate the principles found in healthy, unworn natural dentitions. The design and management of the BMAGO are explicitly dictated by these "optimal biologic dental system principles," with the specific goal of achieving a Stable Condylar Position (SCP).16 While some sources use MAGO and BMAGO interchangeably or in close association 17, the distinction is crucial for an accurate appraisal of the evidence. The primary scientific paper used to validate MAGO therapy is, in fact, about the BMAGO. This report will therefore proceed by treating the principles of both as largely synonymous, as they are presented in the source materials, but will consistently acknowledge that the specific evidence cited originates from research on the "Bioesthetic" variant. This distinction highlights a fundamental disconnect between the marketing of the MAGO and the hierarchy of scientific evidence. The claim of being the "only scientifically proven" therapy is a powerful one, yet it rests on a single retrospective cohort study. In the hierarchy of evidence, an observational cohort study provides a lower level of proof than a Randomized Controlled Trial (RCT), and significantly less than a systematic review or meta-analysis of multiple RCTs. The study's own authors appropriately frame their work as a preliminary investigation intended to justify the need for a future RCT, not as definitive proof of superiority.16 This contrasts sharply with the existence of higher-tier evidence, such as systematic reviews on occlusal splints in general, which present far more cautious or even negative conclusions regarding their long-term efficacy.19 This discrepancy between a marketing narrative built on a single, lower-tier study and the broader, more complex scientific consensus is a central theme in the critical evaluation of this appliance. Moreover, the diagnostic role of the MAGO has profound implications for the overall treatment journey. The appliance is explicitly described as a "stepping stone" and "not a cure".12 Its purpose is to achieve a stable jaw position so that a final diagnosis can be made and definitive treatment can be planned.1 This definitive treatment—such as full-mouth rehabilitation, orthodontics, or crowns—is typically irreversible and represents a significant additional commitment of time and resources.5 Therefore, the successful application of a MAGO does not end treatment; rather, it validates the need for and initiates a more extensive second phase. This dynamic positions the MAGO as a form of "diagnostic Trojan horse": it provides initial, reversible pain relief that builds patient confidence, but its success logically commits the patient to a more comprehensive and permanent treatment plan. This underscores the critical importance of obtaining fully informed consent at the outset, ensuring the patient understands the entire anticipated pathway, not just the initial splint therapy phase.
II. Biomechanical and Neuromuscular Mechanism of Action
The therapeutic effect of the Maxillary Anterior Guided Orthotic is attributed to its ability to fundamentally alter the biomechanical and neuromuscular function of the entire masticatory system. By introducing an idealized, temporary occlusal scheme, the MAGO works to deprogram dysfunctional muscle activity, allow for the orthopedic stabilization of the temporomandibular joints, and facilitate a process of neuromuscular re-education.
2.1 Muscle Deprogramming and Relaxation
The primary mechanism of the MAGO is the immediate disengagement of the posterior teeth.13 The appliance is fabricated with a smooth, flat occlusal surface in the posterior regions and a precisely contoured ramp in the anterior region. When the patient closes their jaw or moves it side-to-side or forward, only the lower incisors make contact with this anterior guidance ramp.13 This design element ensures that the posterior teeth (premolars and molars) are kept completely apart during all movements. This disocclusion is physiologically significant. In a dysfunctional bite, premature or interfering contacts between posterior teeth during jaw closure and movement are thought to be a major source of noxious stimuli to the neuromuscular system. These interferences can trigger hyperactivity in the powerful elevator muscles of the jaw—the masseter, temporalis, and medial pterygoid muscles.24 This sustained hyperactivity leads to muscle fatigue, spasm, ischemia, and pain. The MAGO interrupts this pathological feedback loop. By eliminating all posterior tooth contacts, it removes the source of the occlusal interferences. This process is often referred to as "deprogramming" the muscles.23 The central nervous system no longer receives the signals that trigger the protective, hyperactive muscle response. As a result, the masticatory muscles are allowed to relax, breaking the cycle of spasm and pain.3 Electromyographic (EMG) studies on similar anterior-only contact appliances have suggested that this design can reduce the maximum clenching force of the elevator muscles to as little as 20-30% of their original capacity, dramatically reducing the strain on the entire system.23
2.2 Re-establishing Optimal Condylar Position
The chronic hyperactivity of the masticatory muscles not only causes pain but also holds the mandible in a compromised position, preventing the condyles from seating properly within the glenoid fossae. Once the MAGO has facilitated muscle relaxation, the mandible is freed from this "splinting" effect. Without the influence of the habitual bite forcing the jaw into an accommodated position, the condyles are able to move toward their most orthopedically stable and physiologically sound position.1 This optimal joint position is referred to by several terms within the dental literature, including centric relation (CR), which is defined as the most superior-anterior position of the condyles in the fossae, resting against the posterior slopes of the articular eminences, with the articular discs properly interposed.13 Within the bioesthetic framework associated with the BMAGO, this is termed the Stable Condylar Position (SCP).16 Regardless of the terminology, the goal is to achieve a condylar position that is determined by the anatomy of the joint and the relaxed state of the muscles, rather than by the interdigitation of the teeth. By allowing the joints to reach this stable position, the MAGO effectively "unloads" the TMJ structures, particularly the articular disc and the retrodiscal tissues, from the dysfunctional stresses that can lead to inflammation, internal derangement, perforation, or permanent displacement.13 The appliance does not actively force the jaw into a new position; instead, it creates the ideal conditions for the jaw to find its own natural equilibrium. This mechanism can be conceptualized as a biological "reset button." The existing malocclusion acts as a persistent constraint, holding the entire system in a state of strain. The MAGO temporarily removes this constraint, allowing the condyle-disc-muscle assembly to revert to its most unstrained, physiologically determined state. This explains why the therapy is diagnostic—it reveals the individual's unique, ideal jaw relationship, which was previously masked by the dental malocclusion.
2.3 Alteration of Proprioceptive Input and Neuromuscular Re-education
The teeth are surrounded by the periodontal ligament, which is rich in mechanoreceptors that provide the brain with precise information about tooth contact—a sense known as proprioception. In a malocclusion, this proprioceptive feedback reinforces a dysfunctional pattern of muscle activity, creating a learned neuromuscular pattern, or "engram".23 The MAGO fundamentally alters this sensory input. By replacing the complex landscape of individual tooth contacts with a single, smooth point of contact in the anterior, it effectively erases the old proprioceptive map.23 This change in sensory feedback is a key part of the deprogramming process. Over the course of the therapy, as the patient consistently functions on the idealized surface of the MAGO, a new, healthier neuromuscular pattern begins to form. The brain starts to "reprogram" the muscles to function in coordination with the newly established stable joint position.2 This neuromuscular re-education is crucial for achieving long-term stability. The ultimate goal is to establish a state of "neuromuscular harmony" within the masticatory system, where the muscles, joints, and nervous system are all functioning in a coordinated and unstrained manner, and a mechanical disadvantage is created for parafunctional forces like clenching and grinding.13
III. Clinical Application and Treatment Protocol
The clinical application of the Maxillary Anterior Guided Orthotic involves a systematic protocol that begins with a comprehensive patient assessment and proceeds through appliance fabrication, a highly monitored therapeutic phase, and finally, the transition to definitive treatment. The success of the therapy is highly dependent on both meticulous clinical management and strict patient compliance.
3.1 Patient Assessment and Clinical Indications
The process begins with a thorough diagnostic workup. This includes a detailed patient history and a comprehensive clinical examination, often involving a bite analysis to inspect the teeth, jaw joints, and the function of the chewing muscles.12 The clinician assesses the patient's occlusion, range of motion, and palpates the muscles and joints for tenderness. MAGO therapy is indicated for a range of patients presenting with signs and symptoms of temporomandibular disorders and occlusal instability.13 Specific clinical indications cited in the literature include:
- Pain-related TMD: Chronic jaw pain, facial pain, frequent headaches (including migraines), and earaches.3
- Intra-articular Disorders: Degenerative joint disease and symptoms such as TMJ popping, clicking, or locking.9
- Parafunctional Habits: Management of severe clenching and grinding (bruxism) to protect the dentition and reduce muscle hyperactivity.6
- Pre-Restorative or Pre-Surgical Stabilization: As a preparatory phase to establish a stable and reproducible jaw position before undertaking complex procedures like full-mouth dental rehabilitation or orthognathic surgery.9
3.2 Fabrication and Delivery: Conventional vs. Digital Workflows
The fabrication of a MAGO is a precise process that can be accomplished through either traditional laboratory techniques or modern digital workflows.
3.2.1 Conventional Fabrication
The conventional method is a craft-intensive process reliant on physical models and manual skill.8 1. Impressions and Records: The clinician takes accurate impressions of the maxillary and mandibular arches. A critical step is the capture of an interocclusal record. The mandible is gently manipulated into a desired position, typically centric relation, and a record is made using a material like wax or registration silicone. This record must establish a vertical opening of approximately 1.5 to 2 mm between the posterior teeth to provide adequate thickness for the splint material.26 A deprogramming device, such as a Lucia Jig placed on the anterior teeth, may be used for several minutes prior to taking the record to help relax the elevator muscles and facilitate the manipulation.26 2. Laboratory Articulation and Wax-up: The resulting dental casts are mounted on a semi-adjustable articulator using a facebow transfer to orient the maxillary cast to the patient's cranial landmarks.27 The mandibular cast is then mounted against the maxillary cast using the interocclusal record. 3. Acrylic Processing and Finishing: The splint is fabricated on the maxillary cast using a hard, clear methyl methacrylate resin.8 This can be done using a "salt-and-pepper" technique, where monomer and polymer are applied incrementally, or by processing a doughy mass of acrylic in a pressure pot under heat to ensure a dense, non-porous result.26 After curing, the technician manually grinds, shapes, and polishes the splint to create a flat occlusal surface for the posterior teeth and the precise contours of the anterior guidance ramp.28
3.2.2 Digital (CAD/CAM) Fabrication
The digital workflow leverages advanced imaging and manufacturing technologies to enhance precision and efficiency.31 1. Digital Data Acquisition: Instead of physical impressions, an intraoral scanner is used to create highly accurate 3D digital models of the patient's arches.21 This data can be integrated with Cone Beam Computed Tomography (CBCT) scans of the TMJs and data from electronic jaw motion tracking (JMT) systems. This fusion of data allows for a dynamic, patient-specific 3D simulation of mandibular movement, providing unparalleled diagnostic information.21 2. Virtual Design: The digital models are imported into specialized CAD (computer-aided design) software. The clinician or technician can then virtually design the splint with precise control over every parameter, including thickness, the location of occlusal contacts, and the angle and length of the guidance ramps.28 3. Digital Manufacturing: The final design is sent to a manufacturing unit. The splint is either milled from a solid block of polymethyl methacrylate (PMMA) using a subtractive CAM (computer-aided manufacturing) process or 3D printed using an additive process with a biocompatible resin.28 Digital fabrication has been shown to significantly reduce laboratory working time and clinical adjustment time compared to conventional methods.31 Upon completion, the splint is delivered to the patient. The clinician makes any necessary initial adjustments to ensure it seats fully and passively without rocking, and verifies that the occlusal scheme is correct.8
3.3 The Therapeutic Regimen: Wear Time and Adjustments
The management of the patient during the therapeutic phase is critical to the success of MAGO therapy. This phase is characterized by intensive wear and frequent, meticulous adjustments.
3.3.1 Wear Time
A notable area of inconsistency within the available literature is the recommended wear time. This variation suggests that "MAGO therapy" may not be a single, standardized protocol but rather a general approach with significant practitioner-dependent variables.
- Protocol 1: Continuous 24/7 Wear: Several sources advocate for the most intensive protocol, requiring the MAGO to be worn 24 hours a day, 7 days a week, including while eating.1 The rationale is that this provides constant deprogramming and prevents the patient from reverting to their dysfunctional bite pattern at any point during the day.
- Protocol 2: Full-Time Wear Excluding Meals: An alternative protocol calls for full-time wear (24 hours a day) but instructs the patient to remove the splint for meals and active sports.34
- Protocol 3: Primarily Nocturnal Wear: Other clinicians suggest a less intensive regimen where the splint is worn primarily at night, with potential for some daytime wear as needed.2
This discrepancy is not trivial. The decision to eat with the appliance in place subjects it to immense functional forces and has implications for diet and hygiene. Conversely, removing it for meals reintroduces the original malocclusion multiple times per day, potentially slowing or interfering with the deprogramming process. This lack of a standardized protocol presents a significant challenge for research, making it difficult to compare outcomes across studies if the core therapeutic intervention is applied differently.
3.3.2 Adjustment Schedule and Duration
Regardless of the wear-time protocol, frequent adjustments are a non-negotiable component of the therapy. Patients typically return for follow-up appointments once a week.2 At each visit, the clinician carefully assesses the occlusal contacts on the splint and makes minute adjustments. As the muscles relax and the condyles continue to seat into a more stable position, the way the lower jaw contacts the splint will change. These regular adjustments are necessary to maintain the idealized occlusal scheme and continue guiding the jaw toward its stable endpoint. The initial diagnostic and therapeutic phase of MAGO therapy generally lasts from four to twelve weeks.6 However, the duration is patient-dependent and can extend to three months or more in complex cases.1 The therapy is considered complete when the jaw joint position has fully stabilized.
3.4 Monitoring Progress: The Hinge Axis Recording
The primary objective measure used to determine when stability has been achieved is the hinge axis recording.6 The hinge axis is the rotational center of the condyles. During the weekly adjustment appointments, the clinician records this position. In the early stages of therapy, this recorded position will vary from visit to visit as the muscles deprogram. Stability is confirmed when the clinician is able to record the same, consistent hinge axis position over several consecutive appointments. This reproducibility indicates that the condyles have reached their terminal, stable position and that the diagnostic phase of therapy is complete. At this point, the clinician can confidently proceed with planning the definitive, corrective phase of treatment.
IV. A Critical Appraisal of the Scientific Evidence
The evaluation of any medical or dental therapy requires a rigorous appraisal of the scientific evidence supporting its efficacy. In the case of the Maxillary Anterior Guided Orthotic, the evidence base is characterized by a strong central claim derived from a single cohort study, which must be contextualized within the broader, more complex landscape of research on occlusal splints for temporomandibular disorders.
4.1 The Sletten et al. (2015) Cohort Study on the BMAGO
The cornerstone of the evidence cited by proponents of MAGO therapy is a 2015 retrospective cohort study by Sletten et al., which investigated the effects of the Bioesthetic Maxillary Anterior-Guided Orthosis (BMAGO).15
- Methodology: The study analyzed the records of 157 symptomatic patients treated in a private practice over an eight-year period. These patients presented with a mix of TMD, head, neck, and shoulder pain.16 The treatment protocol required patients to wear the BMAGO 24 hours a day, 7 days a week, with adjustments performed at two-week intervals until a Stable Condylar Position (SCP) was achieved. The average treatment time to stabilization was six months. At each visit, patients rated the intensity of 12 different symptoms on a Numeric Rating Scale (NRS) from 0 to 10.16
- Findings: The study reported a statistically significant improvement ($p < 0.001$) in 11 of the 12 symptoms evaluated. The symptoms showing highly significant reductions included TMJ pop, click, and lock; pain in the jaw, neck, and shoulder; headache and earache; and parafunctional habits like clenching and grinding.16 A dramatic reduction in tinnitus was also observed, though the sample size for this symptom was too small to be statistically predictive.16
- Long-Term Follow-up: A review of the patient records indicated that 90% of the cohort proceeded with definitive dental treatment after stabilization. For the 10% who did not and were instructed to continue wearing the BMAGO nightly for protection, the records reportedly showed "no return of symptoms" after a period of more than eight years.16
- Critical Analysis: While the outcomes reported in the Sletten et al. study are compelling, it is essential to interpret them within the context of the study's design. As a retrospective cohort study, it is an observational design that lacks a control group. This is a significant limitation. Without a control group (e.g., patients receiving a placebo splint or an alternative therapy), it is impossible to definitively attribute the observed improvements solely to the BMAGO. The positive outcomes could be influenced by other factors, such as the placebo effect, the natural waxing and waning course of TMD, or the intensive clinical attention and follow-up the patients received. The authors themselves responsibly position the study not as definitive proof, but as an evidence base sufficient to "warrant BMAGO research in the form of prospective clinical RCTs".16
4.2 Broader Context: Efficacy of Occlusal Splints for TMD (Systematic Reviews & Meta-Analyses)
When the single BMAGO cohort study is placed against the broader scientific literature on occlusal splints for TMD, a more nuanced and less certain picture emerges. General literature reviews often conclude that hard occlusal appliances, as a category, have "good evidence of modest efficacy" in managing painful TMD 16 and can significantly reduce symptoms in the majority of patients.13 However, systematic reviews and meta-analyses, which sit at the top of the evidence hierarchy, provide more cautious conclusions.
- One comprehensive review concluded that there is "no clear evidence that occlusal splints are superior to physiotherapy" for treating TMDs. It also found that in long-term follow-up, splints were "equally effective as other therapies," suggesting they do not offer a unique long-term advantage.13
- A 2020 systematic review and meta-analysis by Fouda et al. presented an even more critical assessment. After analyzing 22 studies, the authors concluded there is "no evidence of the effectiveness of oral splints" in reducing TMJD pain or improving function in either short-term or long-term follow-up.19 Most strikingly, their meta-analysis of long-term studies found that the control groups (receiving therapies like counseling, no treatment, or placebo splints) experienced a statistically significant greater reduction in pain compared to the groups receiving active splint therapy.19
This stark contradiction between the highly positive results of the single BMAGO study and the skeptical conclusions of higher-level meta-analyses is the central challenge in evaluating this therapy. It suggests that while the specific design and meticulous management protocol of the BMAGO may yield positive results in a dedicated clinical setting, the evidence for the general efficacy of splints as a class of treatment is far from settled and may be no better than placebo or other conservative measures in the long run. To better understand the MAGO's place within this landscape, it is useful to compare its design principles to other common splint types. Table 1: Comparative Analysis of Common Occlusal Splint Modalities
Splint Type Design Principles Primary Mechanism of Action Primary Indications Summary of Evidence/Notes (from sources) MAGO / BMAGO Maxillary full-coverage hard acrylic splint with a prominent anterior guidance ramp. 1 Muscle deprogramming via posterior disocclusion; allows condylar seating into a stable orthopedic position (CR/SCP). 13 Myofascial pain, TMD symptoms (headaches, joint noise), bruxism, and as a diagnostic tool before major restorative work. 4 A 2015 cohort study on the BMAGO showed significant reduction in 11 of 12 TMD symptoms. This is the primary evidence cited for its efficacy. 16 Stabilization Splint (Michigan Splint) Maxillary full-coverage hard acrylic splint with a flat occlusal plane and gentle canine guidance. Provides even, simultaneous contacts for all opposing teeth in centric relation. 8 Joint unloading by distributing occlusal forces evenly; reduces muscle hyperactivity by providing an ideal, interference-free occlusion. 13 Myofascial pain, arthralgia (joint pain), bruxism, and occlusal stabilization. 13 Considered a gold standard for stabilization splints. Evidence is mixed but generally shows modest efficacy for myalgia. Strong evidence against its use for TMJ clicking. 36 Anterior Repositioning Splint (ARS) Maxillary or mandibular splint with an anterior ramp that actively postures the mandible forward into a protrusive position. 8 Intentionally alters the condyle-disc relationship, aiming to "recapture" an anteriorly displaced disc and reduce joint clicking and locking. 13 Internal derangements, specifically anterior disc displacement with reduction (reciprocal clicking). 22 Can be effective for short-term symptom control, but prolonged use carries a high risk of causing irreversible, iatrogenic changes to the bite (posterior open bite). Should only be used with extreme caution and for short periods. 8 NTI-tss (Nociceptive Trigeminal Inhibition) Small acrylic device that fits only over the maxillary or mandibular anterior teeth, creating a single point of contact for the opposing incisors. 8 Muscle relaxation via the trigeminal inhibition reflex. The intense stimulation of incisor proprioceptors is thought to reflexively shut down the powerful elevator muscles. 23 Prevention of bruxism, tension-type headaches, and migraines triggered by trigeminal hyperactivity. 8 Prevents posterior teeth from contacting, reducing clenching forces. Carries risks of aspiration, tooth mobility, and occlusal changes with unmonitored long-term use. 8
4.3 Long-Term Outcomes and Post-Therapeutic Stability
The question of long-term efficacy is paramount. The BMAGO cohort study's finding of sustained symptom relief after eight years for patients continuing nightly wear is encouraging, though it applies to a small subset of the original group and is based on a retrospective record review rather than a prospective follow-up study.16 Patient testimonials also support the idea of lasting relief.39 However, the broader literature on splint therapy presents a more cautious outlook on long-term outcomes. While some studies report lasting improvement for the majority of adult patients treated with occlusal appliances 40, others find that TMD symptoms can be persistent or recurrent over many years.40 A meta-analysis by Zhang et al. found that splint therapy did increase mouth opening and reduce pain for certain subgroups but had no significant effect on TMJ clicking.41 The most critical long-term data comes from the Fouda et al. meta-analysis, which, as noted, found that oral splints were not effective for pain or function in the long term, with control groups showing superior pain reduction at the one-year mark.19 This divergence in findings suggests that while a meticulously managed protocol like the one used for the BMAGO may produce positive and stable long-term results, the overall long-term effectiveness of splint therapy as a general treatment modality remains a subject of significant scientific debate.
V. Benefits, Limitations, and Associated Risks
A balanced clinical perspective requires a thorough understanding of not only the potential benefits of a therapy but also its inherent limitations, contraindications, and potential for adverse events. While MAGO therapy is presented as a conservative and effective treatment, it is not without challenges and risks.
5.1 Reported Therapeutic Benefits
Proponents of MAGO therapy highlight several key advantages over other treatment modalities, particularly more invasive procedures.6
- Fast and Effective Symptom Relief: One of the most frequently cited benefits is the rapid alleviation of symptoms. Many patients report a significant reduction in jaw pain, muscle soreness, and headaches within the first two to three weeks of therapy.5 This quick relief can be highly motivating for patients who have been suffering from chronic pain.
- Non-Invasive and Reversible (Initial Phase): The MAGO appliance itself is a removable device that does not require any permanent alteration to the teeth or jaw structures. This makes the initial diagnostic phase of treatment completely non-invasive and, in principle, reversible.6 This conservative approach is a significant advantage compared to surgical interventions or irreversible occlusal adjustments.
- Enhanced Diagnostic Accuracy: Perhaps the most powerful benefit of MAGO therapy is its function as a diagnostic tool. By stabilizing the jaw joints in their optimal physiologic position, it allows the clinician to accurately identify the true source of the patient's dysfunction.1 This process "takes the guesswork out of diagnostics" 2, providing a verifiable blueprint for any subsequent definitive treatment and increasing the predictability of long-term success.
- Improved Masticatory Function: Beyond pain relief, patients often experience a marked improvement in jaw function, including a greater range of motion and more comfortable chewing, speaking, and swallowing.3
5.2 Limitations and Contraindications
Despite its benefits, MAGO therapy has several important limitations and potential contraindications that must be considered.
- Patient Compliance: The success of the therapy is critically dependent on patient compliance. Protocols that require 24/7 wear can be socially and functionally demanding.16 Patients who are unable or unwilling to adhere to the strict wear schedule are unlikely to achieve the desired therapeutic outcome.
- Not a Standalone Cure: It is essential to recognize that MAGO therapy is not a final cure but a diagnostic and transitional phase. The appliance stabilizes the system, but once it is discontinued without follow-up treatment, the original symptoms are likely to return as the teeth guide the jaw back into its dysfunctional position.12 Patients must be prepared to commit to the definitive treatment that is indicated after the MAGO phase is complete.
- Risk of Iatrogenic Occlusal Changes: All occlusal splints, particularly those worn for extended periods, carry an inherent risk of causing unintended and potentially harmful changes to the patient's bite. The National Institutes of Health (NIH) explicitly warns that if a splint is recommended, it should be for a short time and "should not cause permanent changes in the bite".8 Appliances like the MAGO that feature only anterior contact can, if not managed properly, lead to the supra-eruption of the unopposed posterior teeth, creating a posterior open bite that can be very difficult to correct.22 This risk underscores the necessity of close, expert supervision throughout the therapy.
- Cost and Insurance Coverage: Occlusal splint therapy can be a significant financial investment, often costing thousands of dollars for the appliance and the series of adjustment appointments.8 Due to the lack of definitive, large-scale RCTs verifying its efficacy and safety, many medical and dental insurance plans may not provide coverage for the treatment, leaving the patient with the full financial burden.8
5.3 Adverse Events and Patient Safety
While generally considered safe when properly managed, the potential for adverse outcomes exists. The FDA's Manufacturer and User Facility Device Experience (MAUDE) database includes a detailed adverse event report related to a MAGO appliance that serves as a critical cautionary tale.42 According to the report, a 45-year-old female patient with no prior history of TMJ problems was allegedly "forced" by her dentist and orthodontist to wear a MAGO. After nearly five months of use, the patient reported developing significant new symptoms, including "big neck problems," unwanted tooth movement, and an increase in jaw pain. Furthermore, she reported that X-rays showed her airway had become smaller post-treatment. The patient was then told she would need to wear the device for several more years, followed by permanent nightly wear, or her "jaw will collapse," and that she would require extensive restorative work.42 While this is a single case report and cannot be generalized to all patients or practitioners, it is highly instructive. It highlights the potential for serious iatrogenic harm if the therapy is misapplied, used on an inappropriate patient, or not monitored with extreme care. The report of a reduced airway is particularly concerning. This case underscores that a MAGO is not a simple device but a powerful orthopedic tool that can induce significant biological changes. Its use demands a high level of clinical expertise, a thorough initial diagnosis to rule out contraindications, and a commitment to meticulous, ongoing patient monitoring to ensure safety and prevent negative outcomes. If a patient experiences an increase in pain or develops new symptoms, the therapy should be stopped and re-evaluated immediately.8
VI. The MAGO as a Gateway to Definitive Treatment
A core concept that distinguishes MAGO therapy from the simple use of a protective night guard is its explicit role as a preparatory and diagnostic phase for subsequent, definitive dental treatment. The MAGO is not the end of the therapeutic journey; it is the beginning. Its purpose is to create a stable, healthy foundation upon which a permanent, functional, and comfortable occlusion can be built.
6.1 From Diagnosis to Definitive Care
The stable and reproducible jaw position achieved at the conclusion of MAGO therapy is the most critical piece of diagnostic information obtained. This position, representing the harmonious relationship between the condyles and their fossae, becomes the functional and orthopedic "blueprint" for the final treatment plan.1 Once the clinician has verified this stable position, they can accurately diagnose the specific nature of the discrepancy between this ideal joint position and the patient's existing bite. This diagnosis is the key to planning a predictable and successful long-term solution.7 This approach aligns with a fundamental principle of conservative and responsible dentistry: irreversible procedures should not be undertaken until a stable, comfortable, and functional state has been achieved and verified.43 Attempting to perform extensive restorative or orthodontic work on a patient with an unstable jaw joint is highly unpredictable and risks perpetuating or worsening the underlying dysfunction. The MAGO provides a reversible means to "test drive" and confirm the ideal jaw position before committing to permanent changes.
6.2 Pathways Post-Stabilization
After the successful completion of the MAGO phase, the therapeutic goal shifts. The objective is now to permanently alter the patient's dentition so that it supports the mandible in the newly established stable joint position without the need for the orthotic. This ensures that the therapeutic benefits are maintained long-term. There are several pathways to achieve this, and the choice depends on the severity and nature of the diagnosed malocclusion 2:
- Occlusal Equilibration: For minor discrepancies, the clinician may perform a procedure called occlusal equilibration. This involves the highly selective and precise removal of small amounts of tooth enamel from interfering contacts. The goal is to reshape the biting surfaces of the teeth so that they meet evenly and simultaneously when the jaw is in its stable position.2
- Restorative Dentistry: When there are more significant discrepancies, or if teeth are worn or damaged, an additive approach is needed. This involves using restorative materials like composite resin bonding or fabricating crowns and veneers to build the teeth up to the correct shape and height, establishing a new bite that is in harmony with the stable joint position.2
- Orthodontic Treatment: If the teeth are significantly malposed, orthodontics may be the most appropriate definitive treatment. Braces or clear aligners are used to physically move the teeth into positions that create a stable, functional occlusion that supports the healthy joint position.2
- Orthognathic Surgery: In cases where the malocclusion is due to a significant underlying skeletal deformity of the maxilla or mandible, a combination of orthodontics and orthognathic surgery may be required. The surgery physically repositions the jawbones to correct the skeletal discrepancy, establishing the foundation for a stable final occlusion.9
6.3 Integration with Broader Dental Philosophies
MAGO therapy is not a standalone technique but is often a central component of broader, more comprehensive dental philosophies that emphasize a holistic view of the masticatory system.
- Bioesthetic Dentistry: As previously discussed, the BMAGO is the specific appliance used within the framework of Bioesthetic Dentistry. This philosophy is based on emulating the form and function of healthy, natural, and unworn chewing systems. It prioritizes establishing a Stable Condylar Position (SCP) as the absolute foundation before any restorative or esthetic treatment is considered.5 The BMAGO is the primary tool for achieving and verifying this SCP.
- Gneuromuscular (GNM) Dentistry: This philosophy represents a synthesis of traditional gnathological principles (the mechanics of jaw movement) and neuromuscular principles (the physiology of the muscles and nerves). GNM dentistry uses advanced diagnostic tools like jaw tracking and electromyography in conjunction with orthotics to find a physiologic rest position for the mandible and establish an occlusion that is in harmony with the entire system.47 The MAGO, or similar orthotics, plays a key role in this diagnostic and therapeutic process.
In both philosophies, the MAGO serves the same fundamental purpose: to deprogram the system and reveal the ideal, stable foundation from which all other treatment should proceed. This approach contrasts with more traditional dental models that may focus on the teeth in isolation without first ensuring the stability of the underlying TMJs and musculature.1
VII. Conclusion and Expert Recommendations
This comprehensive review has synthesized the available clinical and scientific literature on the Maxillary Anterior Guided Orthotic (MAGO). The analysis reveals that the MAGO is a highly specialized occlusal appliance designed to function as both a therapeutic device for short-term symptom relief and, more critically, as a reversible diagnostic tool for complex occlusal and temporomandibular disorders. Its proposed mechanism of action—utilizing anterior guidance to deprogram masticatory muscles and facilitate the seating of the mandibular condyles into a stable, physiologic position—is well-defined within its theoretical framework and represents a logical clinical approach to managing TMD. The central challenge in evaluating the MAGO lies in reconciling the assertive marketing claims of its unique, scientifically-proven efficacy with the broader body of scientific evidence. The claim that it is the "only" proven splint therapy is predicated almost entirely on a single, non-randomized, retrospective cohort study of the closely related Bioesthetic MAGO (BMAGO). While the positive results of this study are noteworthy, its observational design has inherent limitations and cannot be considered definitive proof of superiority. This stands in stark contrast to higher-level evidence from systematic reviews and meta-analyses on occlusal splints in general, which suggest more modest, less certain, and in some cases, no significant long-term benefits compared to placebo or other conservative therapies. The MAGO's most significant and defensible role appears to be as a gateway to definitive treatment. It provides a non-invasive method to stabilize the masticatory system, thereby enabling an accurate diagnosis of the underlying etiology of the patient's dysfunction. This diagnostic clarity is invaluable before proceeding with irreversible and costly treatments such as full-mouth rehabilitation or orthodontics. However, this also means that the MAGO is not a final cure but the first step in a much larger therapeutic process, a fact that must be clearly communicated to patients. Based on this comprehensive analysis, the following recommendations are offered for clinicians and researchers.
Recommendations for Clinicians:
1. Prioritize the Diagnostic Function: The MAGO should be utilized primarily as a diagnostic instrument. Its greatest clinical value lies in its ability to determine and verify a stable, physiologic condylar position before irreversible treatment is planned. The therapeutic relief it provides should be viewed as confirmation of a correct diagnostic path. 2. Ensure Comprehensive Informed Consent: Given that MAGO therapy is a precursor to more extensive treatment, clinicians have an ethical obligation to ensure patients provide fully informed consent for the entire anticipated treatment pathway at the outset. This includes a transparent discussion of the potential subsequent treatments (e.g., equilibration, orthodontics, restoration), their irreversible nature, and the total estimated costs and timelines. 3. Adhere to Meticulous Monitoring and Adjustment: The potential for adverse outcomes, as highlighted by the FDA MAUDE report and general warnings about prolonged splint use, necessitates rigorous clinical oversight. Close and frequent monitoring, including the recommended weekly adjustments, is not optional but is an essential component of patient safety and therapeutic success. Any increase in pain or development of new symptoms should prompt an immediate cessation and re-evaluation of the therapy.
Recommendations for Future Research:
There is a clear and pressing need for high-quality, independent research to validate the specific claims made about the MAGO/BMAGO design. Future studies should be designed to address the current evidentiary gaps: 1. Conduct Randomized Controlled Trials (RCTs): High-quality RCTs are essential. These trials should directly compare the MAGO/BMAGO design against other common splint types (e.g., flat-plane stabilization splints) and credible control groups (e.g., non-occluding placebo splints, physiotherapy, or cognitive-behavioral therapy). 2. Standardize Treatment Protocols: To ensure the comparability and reproducibility of results, future research must utilize and clearly define a standardized clinical protocol, particularly regarding the contentious issue of wear time (i.e., 24/7 wear including or excluding meals). 3. Incorporate Long-Term Follow-up: Studies must include robust, long-term follow-up (ideally several years) to assess the stability of symptom relief and the success of the definitive treatments that the MAGO phase is designed to guide. Only through such rigorous scientific investigation can the specific contributions of the MAGO's anterior-guided design be definitively separated from the general placebo effects and non-specific benefits common to all occlusal appliance therapies. Nguồn trích dẫn 1. MAGO Therapy – Chittenden Dental + Wellness, truy cập vào tháng 10 24, 2025, https://chittendendental.com/magotherapy/ 2. MAGO Splint | Centennial, CO – Rippe Dental Associates, truy cập vào tháng 10 24, 2025, https://www.drrippe.com/mago-splint 3. MAGO TMJ Treatment Shelburne VT | Jaw Pain Relief, truy cập vào tháng 10 24, 2025, https://www.shelburnevillagedentistry.com/mago-tmj-treatment.html 4. Orthoticss — David Clark, DDS | Migraine & TMJ Disorder Treatment | Plano, TX, truy cập vào tháng 10 24, 2025, http://www.davidclarkdds.com/orthotics 5. The Real Truth About MAGO Therapy from My Perspective – Chittenden Dental + Wellness, truy cập vào tháng 10 24, 2025, https://chittendendental.com/the-real-truth-about-mago-therapy-from-my-perspective/ 6. TMJ/TMD Health – Dr. Howard Dean, truy cập vào tháng 10 24, 2025, https://www.drhowarddean.com/tmjtmd-health/ 7. MAGO Splint Therapy for TMJ Patients – Gallagher Dentistry & Facial Pain Center, truy cập vào tháng 10 24, 2025, https://www.gallaghercosmeticdentistry.com/tmj-health-tmd/mago-splint-therapy-for-tmj-patients/ 8. Splints – The TMJ Association, truy cập vào tháng 10 24, 2025, https://tmj.org/living-with-tmj/treatments/splints/ 9. Maxillary Anterior Guided Orthotic: (MAGO) in Menlo Park, CA | Katherine A. Brown, D.D.S, truy cập vào tháng 10 24, 2025, https://menloathertondentist.com/maxillary-anterior-guided-orthotic-mago/ 10. Effective MAGO Therapy in Oxford, MI | John Khoury Dental, truy cập vào tháng 10 24, 2025, https://johnkhourydental.com/dental-services/obi/mago-therapy/ 11. Occlusal Splints for TMD – Dr. Robin Ferguson, truy cập vào tháng 10 24, 2025, https://robinfergusondds.com/occlusal-splints-for-tmd/ 12. TMJ Dentist Dallas | Facial Pain & TMJ Disorder | Dallas TMJ Relief – Segulyev Dental Arts, truy cập vào tháng 10 24, 2025, https://www.segulyevdentalarts.com/tmj-dentist-dallas/ 13. Occlusal splints-types and effectiveness in temporomandibular … – NIH, truy cập vào tháng 10 24, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC9931504/ 14. FREE TMJ Consultation & $250 OFF TMJ Treatment Plan – Dr. Segulyev, truy cập vào tháng 10 24, 2025, https://www.segulyevdentalarts.com/2023/07/26/free-tmj-consultation-250-off-tmj-treatment-plan/ 15. Proven TMJ Relief with MAGO Therapy – Gallagher Dentistry …, truy cập vào tháng 10 24, 2025, https://www.gallaghercosmeticdentistry.com/tmj-health-tmd/proven-tmj-relief-with-mago-therapy/ 16. The effect of specially designed and managed occlusal devices on …, truy cập vào tháng 10 24, 2025, https://www.bioesthetics.com/sites/default/files/newspdf/appliance_therapy.pdf 17. The effect of specially designed and managed occlusal devices on …, truy cập vào tháng 10 24, 2025, https://pubmed.ncbi.nlm.nih.gov/29191153/ 18. mago Archives – Los Angeles Holistic Dentist Boyajian – Dental Wellness Arts, truy cập vào tháng 10 24, 2025, https://dentalwellnessarts.com/tag/mago/ 19. (PDF) No evidence of the effectiveness of oral splints in the …, truy cập vào tháng 10 24, 2025, https://www.researchgate.net/publication/338013384_No_evidence_of_the_effectiveness_of_oral_splints_in_the_management_of_temporomandibular_joint_dysfunction_pain_in_both_short_and_long-term_follow_up_-systematic_review_and_meta-analysis_study 20. Bruxism ☑️ Stomatologia Estetyczna i Ortodoncja Meritum, truy cập vào tháng 10 24, 2025, https://meritum.lodz.pl/en/bruxism/ 21. The fabrication of a customized occlusal splint based on the merging …, truy cập vào tháng 10 24, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC5508405/ 22. Oral splint for temporomandibular joint disorders with revolutionary fluid system – PMC, truy cập vào tháng 10 24, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC3760352/ 23. Guardians of the temporomandibular joint: The occlusal splints- an overview – Arch Dent Res – Archives of Dental Research, truy cập vào tháng 10 24, 2025, https://adr.org.in/archive/volume/12/issue/2/article/771 24. Occlusal splint therapy in TMD pain management: A review – Journal of Global Oral Health, truy cập vào tháng 10 24, 2025, https://jglobaloralhealth.org/occlusal-splint-therapy-in-tmd-pain-management-a-review/ 25. TMJ, Splint Therapy & Occlusion (Bite) – Elevation Dental, truy cập vào tháng 10 24, 2025, https://www.elevationdental.net/tmj-splint-therapy-occlusion-bite 26. (PDF) How to Make a Well-Fitting Stabilization Splint – ResearchGate, truy cập vào tháng 10 24, 2025, https://www.researchgate.net/publication/5896550_How_to_Make_a_Well-Fitting_Stabilization_Splint 27. CAUGHEY splint fabrication.key, truy cập vào tháng 10 24, 2025, https://caugheydds.com/wp-content/uploads/2015/08/CAUGHEY-splint-fabrication.pdf 28. A new computer-assisted method for design and fabrication of occlusal splints | ORTOFACE, truy cập vào tháng 10 24, 2025, https://ortoface.com/wp-content/uploads/2022/05/9_A-new-computer-assisted-method-for-design-and-fabrication-of-occlusal-splints.pdf 29. Construction of an Occlusal Bite Splint – YouTube, truy cập vào tháng 10 24, 2025, https://www.youtube.com/watch?v=NUxqD02u9CQ 30. Splint Fabrication – YouTube, truy cập vào tháng 10 24, 2025, https://www.youtube.com/watch?v=0Bnz_cc5YEQ 31. Comparative Efficacy of Digital 3D‐Printed and Conventional Stable Occlusal Splints in the Treatment of Temporomandibular Disorders – PubMed Central, truy cập vào tháng 10 24, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC12426461/ 32. Dental splints: All about grinding splints, bite splints and more | Alpine BioDental, truy cập vào tháng 10 24, 2025, https://alpine-biodental.ch/en/blog/category/splints/ 33. Comparative Analysis between Conventional Acrylic, CAD/CAM Milled, and 3D CAD/CAM Printed Occlusal Splints – MDPI, truy cập vào tháng 10 24, 2025, https://www.mdpi.com/1996-1944/16/18/6269 34. Splint therapy and when to wear | Prevent grinding | We serve the La Mesa, El Cajon, Spring Valley, Rancho San Diego, and the San Diego, California area – Stormberg Orthodontics, truy cập vào tháng 10 24, 2025, https://orthosandiego.com/instructions/splint-therapy/ 35. No evidence on the effectiveness of oral splints for the management of temporomandibular joint dysfunction pain in both short and long-term follow-up systematic reviews and meta-analysis studies, truy cập vào tháng 10 24, 2025, https://www.jkaoms.org/journal/view.html?doi=10.5125/jkaoms.2020.46.2.87 36. Recommendations on the Use of Oral Orthotic Occlusal Appliance Therapy for Temporomandibular Joint Disorders: Current Evidence and Clinical Practice – PubMed Central, truy cập vào tháng 10 24, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC10390439/ 37. Study Details | NCT06377475 | Fabrication and Insertion of Michigan Splints by Dental Students | ClinicalTrials.gov, truy cập vào tháng 10 24, 2025, https://clinicaltrials.gov/study/NCT06377475 38. An Overview of Anterior Repositioning Splint Therapy for Disc Displacement-related Temporomandibular Disorders, truy cập vào tháng 10 24, 2025, https://ss.bjmu.edu.cn/Sites/Uploaded/File/2022/02/186378077612053408449597182.pdf 39. Another TMJ Success Story with MAGO Therapy – Gallagher Dentistry & Facial Pain Center, truy cập vào tháng 10 24, 2025, https://www.gallaghercosmeticdentistry.com/tmj-health-tmd/another-tmj-success-story-with-mago-therapy/ 40. Long-term treatment outcome for adolescents with temporomandibular pain Kerstin Wahlund1 Bo Larsson2 – NTNU Open, truy cập vào tháng 10 24, 2025, https://ntnuopen.ntnu.no/ntnu-xmlui/bitstream/handle/11250/2590381/Wahlund.pdf?sequence=4 41. Efficacy of splint therapy for the management of temporomandibular …, truy cập vào tháng 10 24, 2025, https://www.oncotarget.com/article/13059/text/ 42. MAUDE Adverse Event Report: MAGO (MAXILLARY ANTERIOR …, truy cập vào tháng 10 24, 2025, https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfmaude/detail.cfm?mdrfoi__id=17870560&pc=OCO 43. MyoalignerR: An innovative approach to Occlusion, TMD and Airway Treatment: A case Study | Published in Advanced Dental Technologies & Techniques, truy cập vào tháng 10 24, 2025, https://adtt.scholasticahq.com/article/122450-myoaligner-an-innovative-approach-to-occlusion-tmd-and-airway-treatment-a-case-study 44. CG-SURG-09 Temporomandibular Disorders, truy cập vào tháng 10 24, 2025, https://www.anthem.com/medpolicies/abcbs/active/gl_pw_a051149.html 45. Indications for Orthognathic Surgery – AAOMS, truy cập vào tháng 10 24, 2025, https://aaoms.org/wp-content/uploads/2025/01/ortho_indications.pdf 46. Indications and Management Protocol for the Use of Splints with the "Surgery First" Approach – Journal of Clinical Orthodontics, truy cập vào tháng 10 24, 2025, https://www.jco-online.com/archive/2021/08/463-overview-indications-and-management-protocol-for-the-use-of-splints-with-the-surgery-first-approach/ 47. (PDF) Physiological State of Occlusal Orthotics and the Diagnosis of Myogenous Orofacial Pain in reducing TMD Headaches and other Symptoms – ResearchGate, truy cập vào tháng 10 24, 2025, https://www.researchgate.net/publication/342332069_Physiological_State_of_Occlusal_Orthotics_and_the_Diagnosis_of_Myogenous_Orofacial_Pain_in_reducing_TMD_Headaches_and_other_Symptoms