Phân tích CBCT và các mốc giải phẫu
Anatomic Landmarks and Systematic Analysis of Dental Cone Beam Computed Tomography The Role of Cone Beam Computed Tomography in Maxillofacial Diagnostics Cone Beam Computed Tomography (CBCT) represents a paradigm shift in maxillofacial imaging, transitioning diagnostic capabilities from the constraints of two-dimensional (2D) representations to the comprehensive spatial understanding afforded by three-dimensional (3D) volumetric data. This technology has become an indispensable tool across nearly every dental specialty, providing clinicians with unparalleled visualization of osseous structures, nerve pathways, and airway spaces. However, its effective and responsible use requires a thorough understanding of its underlying principles, clinical applications, and inherent limitations. Principles of Cone Beam Volumetric Imaging The fundamental technology of CBCT differs significantly from both conventional 2D radiography and medical-grade multi-detector computed tomography (MDCT). A CBCT scanner utilizes a cone-shaped or pyramidal X-ray beam that, in a single 180- or 360-degree rotation around the patient's head, captures a complete volumetric dataset. This single-pass acquisition contrasts sharply with the fan-shaped beam of an MDCT scanner, which requires numerous rotations to acquire a series of individual "slices" that are then stacked to create a 3D volume. During the CBCT scan, the X-ray beam passes through tissues of varying densities, and the attenuated photons are captured by a flat-panel detector. This process generates a sequence of 2D "basis images". A computer then applies sophisticated algorithms to reconstruct these basis images into a three-dimensional matrix of volumetric pixels, or "voxels". A key advantage of CBCT is that these voxels are typically isotropic, meaning they have equal dimensions in all three planes. This geometric accuracy allows for distortion-free, 1:1 measurements of anatomical structures, a capability not possible with 2D radiographs, which are inherently subject to magnification, distortion, and the superimposition of anatomical structures. When compared to MDCT, CBCT offers several distinct advantages for dentomaxillofacial applications. It provides higher spatial resolution for evaluating mineralized structures, a significantly lower radiation dose (approximately 10 times less than a comparable medical CT), shorter scan times, and is produced by smaller, less expensive machines suitable for in-office installation. The primary limitation of CBCT, however, is its poor soft-tissue contrast, which makes it unsuitable for the detailed evaluation of muscles, glands, lymph nodes, or soft-tissue tumors, for which MDCT or Magnetic Resonance Imaging (MRI) remain the modalities of choice. The very accessibility that makes CBCT a powerful in-office tool—its lower cost and smaller footprint—has also given rise to a new challenge in clinical practice. The technology has become widely available to practitioners who may not have received the specialized training required for comprehensive 3D volume interpretation. This creates a potential "diagnostic responsibility gap" between the vast amount of anatomical data captured and the clinical information that is actually extracted. Professional guidelines and the standard of care mandate that the clinician who acquires or interacts with a CBCT volume is responsible for interpreting the entire dataset, not just the primary area of interest. Studies have shown that oral and maxillofacial radiologists identify substantially more incidental findings than general clinicians, highlighting the need for either advanced training or routine collaboration with radiology specialists to ensure that critical diagnostic information is not overlooked. Therefore, the integration of CBCT into a practice represents not merely a technological upgrade but a fundamental evolution of the diagnostic workflow and its associated medico-legal responsibilities. Radiation Safety and the ALARA Principle While the radiation dose from CBCT is considerably lower than that of MDCT, it is still significantly higher than conventional 2D dental imaging. A single CBCT scan can deliver a radiation dose approximately eight times that of a standard panoramic radiograph. This fact underscores the critical importance of adhering to the ALARA (As Low As Reasonably Achievable) principle. The ALARA principle dictates that CBCT should never be used as a routine screening tool. Its use is only justified when a clear clinical objective has been established prior to the scan, and when the anticipated diagnostic information cannot be obtained from lower-dose imaging modalities. The selection of the smallest possible Field of View (FOV) that covers the region of interest is a key component of dose reduction and responsible imaging practice. Broad Spectrum of Clinical Applications The diagnostic power of CBCT has been leveraged across a wide array of dental and maxillofacial disciplines, transforming treatment planning from an exercise in estimation to one of precision. Feature 2D Radiography (Periapical/Panoramic) Cone Beam CT (CBCT) Medical CT (MDCT) Principle Single static X-ray projection Single rotation with a cone-shaped beam Multiple rotations with a fan-shaped beam Dimensionality 2-Dimensional 3-Dimensional 3-Dimensional Radiation Dose Low Moderate (higher than 2D, lower than MDCT) High Spatial Resolution (Hard Tissue) Good Excellent (sub-millimeter isotropic voxels) Good Soft Tissue Contrast Poor Very Poor Good Key Advantages Low cost, low dose, widely available High hard tissue resolution, geometric accuracy, lower dose than MDCT, in-office capability Excellent soft tissue contrast, wide availability in hospitals Key Limitations Superimposition, magnification, distortion Poor soft tissue contrast, susceptible to metallic artifacts High radiation dose, higher cost, larger machine footprint Primary Clinical Use Case Routine dental screening, caries detection, periodontal assessment Dentoalveolar and maxillofacial osseous diagnosis and surgical planning Soft tissue pathology, complex craniofacial trauma, oncologic staging
- Implantology: CBCT is the standard of care for pre-surgical implant planning. It allows for precise, multi-planar assessment of bone height and width, evaluation of bone quality, localization of vital structures like the mandibular canal and maxillary sinus, and fabrication of surgical guides for accurate implant placement.
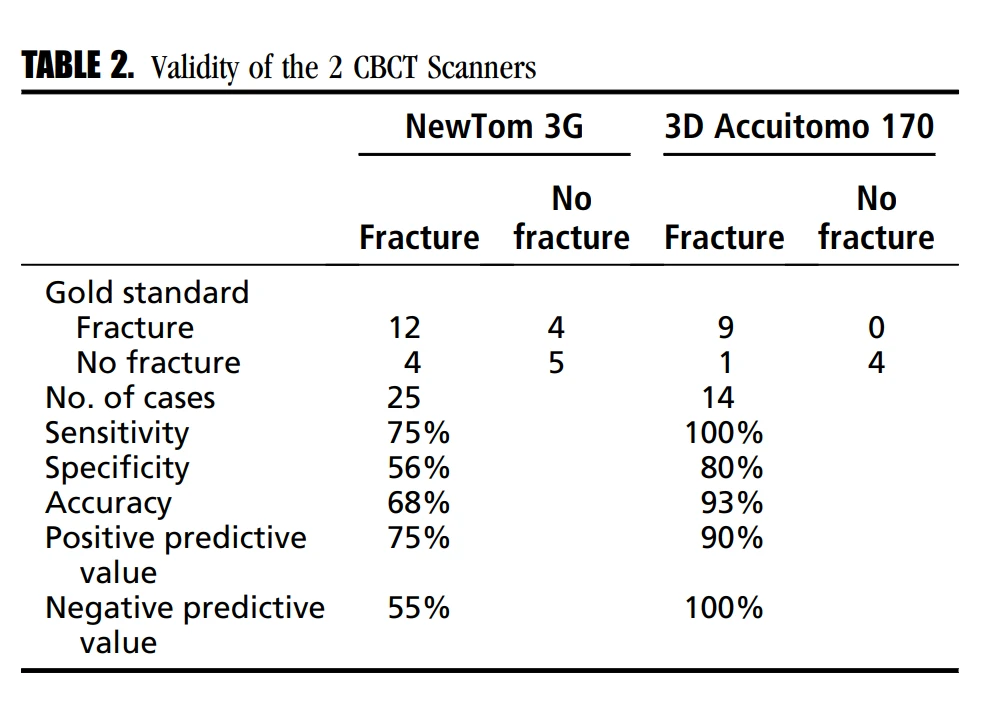
- Oral and Maxillofacial Surgery: The technology is invaluable for assessing maxillofacial trauma, particularly midfacial and orbital fractures, where it provides clear visualization without structural superimposition. It is also used for localizing impacted teeth, planning orthognathic surgery, and evaluating the extent of pathological lesions such as cysts and tumors.
- Endodontics: For complex cases, CBCT can reveal intricate root canal anatomy (e.g., additional canals, C-shaped canals), diagnose vertical root fractures, and assess the size and extent of periapical lesions that may be ambiguous on 2D films.
- Orthodontics and TMJ Disorders: CBCT is used for comprehensive airway analysis, assessment of skeletal asymmetries, accurate localization of impacted teeth for guided eruption, and evaluation of the osseous components of the temporomandibular joint (TMJ), including the mandibular condyle and glenoid fossa.
- Airway Analysis: The volumetric data from CBCT allows for quantitative assessment of the nasopharyngeal and oropharyngeal airway spaces, which is critical in the diagnosis and treatment planning for conditions like obstructive sleep apnea (OSA).
A Systematic Approach to CBCT Volume Interpretation The diagnostic power of a CBCT scan is contingent upon a rigorous and reproducible interpretation methodology. A haphazard review focused only on the primary area of interest is insufficient and fails to meet the standard of care. A systematic approach ensures that all available diagnostic information is evaluated, minimizing the risk of missed pathology and enhancing patient safety. Pre-analysis: Scan Acquisition and Quality Assurance The interpretation process begins before the analysis software is even opened. Proper scan acquisition is foundational to diagnostic quality.
- Patient Preparation: The patient should be instructed to remove any metallic objects from the head and neck region, including jewelry, eyeglasses, hearing aids, and removable dental prostheses, as these can cause significant streak artifacts that obscure anatomical detail.
- Protocol Selection: The clinician must select an imaging protocol—specifically the Field of View (FOV) and voxel resolution—that is appropriate for the diagnostic task at hand, adhering to the ALARA principle. A small, high-resolution FOV is suitable for evaluating a few teeth in endodontics, whereas a large FOV is necessary for orthodontic or airway analysis.
- Quality Control: Immediately following the scan, a preliminary review should be conducted while the patient is still present. This is to check for motion artifacts, which appear as blurring or double margins on the reconstructed images. If significant motion has occurred, the scan should be retaken to ensure diagnostic integrity. The presence and severity of metallic artifacts from restorations or implants should also be noted, as they can render adjacent areas non-diagnostic.
Data Orientation: The Multi-Planar Reconstruction (MPR) Environment Once a quality scan is acquired, the first step in the software is to establish a consistent anatomical frame of reference by orienting the dataset within the multi-planar reconstruction (MPR) views.
- The Orthogonal Planes: The CBCT data is presented in three interconnected, perpendicular planes:
- Axial Plane: This transverse, or "bird's-eye," view is generated as if looking down the patient's head. It is indispensable for assessing buccolingual width, symmetry, and the cross-sectional shape of structures.
- Coronal Plane: This frontal view, as if looking at the patient face-to-face, is optimal for evaluating vertical height, the nasal cavity, and the paranasal sinuses.
- Sagittal Plane: This side view provides a profile of the anatomy, crucial for assessing anteroposterior relationships, such as skeletal class and the trajectory of the incisive canal.
- Reorientation Protocol: Before any diagnostic assessment begins, the dataset must be virtually reoriented. The occlusal plane should be leveled to be parallel with the horizontal plane, and the patient's anatomical midline should be aligned with the software's midline in the axial and coronal views. This simple but critical step ensures that structures can be evaluated for symmetry and prevents misinterpretations caused by a tilted or rotated view.
The Systematic Review: A Comprehensive Full-Volume Workflow The professional, ethical, and medico-legal standard of care requires the interpreting clinician to review the entire scanned volume, regardless of the initial reason for the scan. The American Academy of Oral and Maxillofacial Radiology (AAOMR) has affirmed that the clinician is responsible for all findings within the acquired FOV. Adopting a consistent, reproducible workflow is the most effective way to meet this obligation. A "top-to-bottom" or "outside-in" approach is recommended. An example of a systematic review algorithm is as follows : 1. Cranial Base and Superior Structures: Begin by scrolling through the axial slices from the superior-most extent of the FOV. Examine the visible portions of the cranial base, including the sphenoid and ethmoid bones, and note the pneumatization of the mastoid air cells. 2. Nasal Cavity and Paranasal Sinuses: Continue inferiorly, evaluating the frontal, ethmoid, sphenoid, and maxillary sinuses. Assess for mucosal thickening, fluid levels (air-fluid levels), polyps, retention pseudocysts, and the patency of the ostiomeatal complexes. Note anatomical variations such as a deviated nasal septum or concha bullosa. 3. Orbits and Zygomatic Complex: Examine the integrity of the orbital floors and medial walls, as well as the zygomatic arches. 4. Maxilla and Dentition: Systematically review the maxilla, including the hard palate and maxillary tuberosities. Inspect each maxillary tooth for periapical pathology, root morphology, fractures, and resorption. Note the relationship of posterior tooth roots to the floor of the maxillary sinus. 5. Mandible and TMJs: Evaluate the temporomandibular joints, assessing the morphology of the condylar heads and glenoid fossae. Trace the course of the mandibular canal bilaterally from the mandibular foramen to the mental foramen. Inspect each mandibular tooth. 6. Airway and Soft Tissues: Assess the patency and dimensions of the nasopharynx and oropharynx. Examine the visible soft tissue spaces, such as the parapharyngeal and submandibular spaces, for asymmetries or masses. 7. Cervical Spine: At the inferior extent of the FOV, examine the visible portions of the cervical vertebrae for degenerative changes, anomalies, or fractures. This systematic process forces a cognitive transition. The practitioner is no longer solely a "dentist" focused on a single tooth but becomes a regional diagnostician actively screening for a wide range of pathologies. This shift elevates the role of the dental CBCT scan from a mere pre-surgical tool to a comprehensive head and neck health screening. Consequently, the dental practice can become a crucial, and sometimes unintentional, point of entry into the broader healthcare system for patients with non-dental conditions. A patient presenting for a dental implant evaluation might leave with a life-saving referral to a cardiologist due to the incidental discovery of carotid artery calcifications. The Critical Role of Incidental Findings Incidental findings are abnormal findings discovered during the review that are unrelated to the original purpose of the scan. Their prevalence is remarkably high, reported in up to 93% of CBCT scans, and they are far more identifiable in 3D imaging than in 2D radiographs. The clinical impact of these findings can be profound, ranging from modifications of the dental treatment plan to the discovery of life-threatening diseases.
- Vascular Pathologies: Calcifications in the carotid arteries, visible as radiopacities in the soft tissues of the neck, are a sign of atherosclerosis and a significant risk factor for stroke. Their identification on a dental CBCT scan warrants immediate referral to the patient's physician for further evaluation.
- Malignancies: In a case reported in the literature, a CBCT scan acquired to evaluate a single tooth revealed a lesion in the incisive canal area that was subsequently biopsied and identified as metastasis from prostate cancer.
- Airway and Sinus Disease: Chronic sinusitis, mucosal thickening, retention pseudocysts, and significant airway constriction are common incidental findings that may require referral to an otolaryngologist.
All findings, both primary and incidental, must be thoroughly documented in the patient's record. When a finding is outside the clinician's area of expertise, a differential diagnosis should be considered, and a consultation with or referral to an Oral and Maxillofacial Radiologist is the appropriate and necessary course of action. Anatomic Atlas of the Maxillofacial Region in CBCT A proficient interpretation of CBCT volumes is predicated on a comprehensive, three-dimensional understanding of normal anatomy and its common variations. The textbook concept of a single "normal" anatomy is a clinical oversimplification; CBCT reveals a spectrum of morphology for nearly every landmark. The true clinical value of CBCT lies not just in confirming the presence of a structure but in defining its patient-specific size, shape, and spatial relationships. This detailed anatomical knowledge is the foundation of personalized and safe surgical planning. The following sections provide a detailed atlas of key landmarks, organized by anatomical region. Landmark Name No. Concise Anatomical Description Primary CBCT View(s) Core Clinical Significance Mandibular Structures
Mandible 29 The U-shaped lower jaw bone. All Foundation for lower dentition; site of numerous surgical procedures. Mandibular Ramus 34 The vertical portion of the mandible. Sagittal, Coronal Site for orthognathic surgery (BSSO); common donor site for bone grafts. Coronoid Process 4 Triangular bony projection from the anterior ramus. Sagittal Attachment for temporalis muscle; relevant in trauma and as a graft source. Mandibular Condyle 31 Articulating process of the mandible in the TMJ. Sagittal, Coronal Key structure in TMD diagnosis, orthognathic surgery, and trauma. Mandibular Notch 33 Concavity between the condyle and coronoid process. Sagittal Transmits masseteric nerve/vessels; landmark for ramus surgery. Mandibular Canal 30 Canal within the mandible housing the inferior alveolar nerve. Panoramic, Cross-sectional Critical vital structure to avoid during implant surgery and extractions. Mandibular Foramen 32 Opening on the medial ramus for the mandibular canal. Coronal, Axial Target for inferior alveolar nerve block; landmark for ramus osteotomies. Mental Foramen 39 Opening on the lateral body of the mandible for the mental nerve. All Critical vital structure to avoid during implant and periapical surgery. Genial Tubercle 13 Bony spines on the lingual aspect of the anterior mandible. Sagittal, Axial Muscle attachment site; relevant for OSA surgery and anterior implants. Retromolar Trigone 63 Mucosal area posterior to the last mandibular molar. Axial Important site in oral cancer diagnosis and prosthodontics. Maxillary & Palatal
Maxilla 35 Paired upper jaw bones forming the midface. All Foundation for upper dentition; involved in sinus and orbital anatomy. Maxillary Tuberosity 37 Rounded prominence posterior to the last maxillary molar. Sagittal, Axial Key for denture stability, pterygoid implants, and orthodontic anchorage. Hard Palate 18 Bony roof of the mouth. Coronal, Sagittal Site for orthodontic miniscrews; separates oral and nasal cavities. Middle Suture of Hard Palate 41 Midline suture of the palate. Axial Maturation stage determines approach for maxillary expansion. Incisive Canal 20 Neurovascular channel in the anterior midline maxilla. Sagittal, Axial Critical structure to avoid during anterior maxillary implant placement. Incisive Foramen 21 Oral opening of the incisive canal. Sagittal, Axial Landmark for nasopalatine nerve block and implant planning. Greater Palatine Canal 15 Channel transmitting the greater palatine nerve/vessels. Coronal, Sagittal Landmark for greater palatine nerve block and palatal surgery. Lesser Palatine Canal 28 Smaller channels posterior to the greater palatine canal. Coronal, Sagittal Transmits nerves to the soft palate and tonsil region. Anterior Nasal Spine 1 Midline bony projection at the base of the nasal aperture. Sagittal, Coronal Landmark for implant planning and assessing facial aesthetics. Zygoma 66 The cheekbone. Coronal, Axial Key structure in midface trauma (ZMC fractures) and zygomatic implants. Zygomatic Arch 67 Bony arch formed by zygomatic and temporal bones. Axial Defines facial width; important in trauma assessment and aesthetics. Cranial Base & Sphenoid
Frontal Bone 11 Bone forming the forehead and superior orbit. All Site of frontal sinus; involved in major craniofacial trauma and surgery. Sphenoid Bone 55 Complex "bat-shaped" bone at the cranial base. All Central bone of the skull base, housing numerous vital foramina. Greater Wing of Sphenoid 16 Lateral projection of the sphenoid bone. Coronal, Axial Forms part of the orbit and middle cranial fossa; contains key foramina. Pterygoid Process 53 Inferior projection from the sphenoid bone. Coronal, Axial Landmark for Le Fort osteotomies; origin for masticatory muscles. Medial Pterygoid Plate 38 Medial component of the pterygoid process. Coronal, Axial Forms lateral wall of nasopharynx; origin for tensor veli palatini. Lateral Pterygoid Plate 27 Lateral component of the pterygoid process. Coronal, Axial Origin for pterygoid muscles; critical in TMJ function. Hamulus of Medial Pterygoid Plate 17 Hook-like projection from the medial pterygoid plate. Coronal, Axial Can be a source of orofacial pain if elongated (Eagle's syndrome). Pterygoid Fossa 52 Fossa between the medial and lateral pterygoid plates. Axial Contains medial pterygoid and tensor veli palatini muscles. Foramen Ovale 9 Opening in the greater wing of the sphenoid. Axial, Coronal Transmits the mandibular nerve (CN V3); skull base landmark. Foramen Rotundum 10 Opening in the greater wing of the sphenoid. Axial, Coronal Transmits the maxillary nerve (CN V2); skull base landmark. Carotid Canal 2 Passage for the internal carotid artery in the temporal bone. Axial Not always fully visible; calcifications in the artery are a critical finding. Glenoid Fossa 14 Articulating surface for the mandibular condyle in the TMJ. Sagittal, Coronal Morphology is essential for TMD diagnosis and treatment planning. Styloid Process 59 Slender bony projection from the temporal bone. Coronal, 3D Elongation can cause pain and vascular compression (Eagle Syndrome). External Auditory Canal 8 Bony and cartilaginous canal leading to the eardrum. Coronal, Axial Anterior wall is adjacent to the TMJ and can be fractured in trauma. Dens Axis 6 Odontoid process of the second cervical vertebra (C2). Sagittal, Coronal Important incidental finding for trauma or developmental anomalies. Hyoid Bone 19 U-shaped bone in the neck supporting the tongue. Sagittal, Coronal Position is critical for airway patency and OSA assessment. Nasal, Sinus & Orbital
Nasal Cavity Airway 43 Air-filled space of the nose. Coronal, Sagittal Assessed for patency and volume in breathing disorders. Nasal Bone 42 Paired bones forming the bridge of the nose. Sagittal, Coronal Most commonly fractured facial bone. Nasal Septum 44 Midline partition of the nasal cavity. Coronal, Axial Deviations can cause airway obstruction. Vomer 65 Bone forming the postero-inferior part of the nasal septum. Sagittal, Coronal Midline landmark; agenesis is a rare congenital anomaly. Perpendicular Plate of Ethmoid 51 Bone forming the supero-posterior part of the nasal septum. Coronal, Sagittal Landmark in septoplasty and skull base surgery. Crista Galli 5 Superior projection from the ethmoid bone. Coronal Attachment for falx cerebri; pneumatization is a common variant. Concha Bullosa 3 Pneumatization (air cell) within a nasal concha. Coronal Anatomical variant that may obstruct sinus drainage pathways. Inferior/Middle Meatus 22/40 Spaces under the nasal conchae for sinus drainage. Coronal Key areas in assessing sinus health and pathology. Paranasal Sinuses 7,12,36,56 Air-filled cavities (Frontal, Ethmoid, Maxillary, Sphenoid). All Commonly show incidental pathology (e.g., mucosal thickening). Sphenoid Sinus Septum 57 Bony partition(s) within the sphenoid sinus. Coronal, Axial Highly variable; critical landmark for transsphenoidal surgery. Orbit 48 Bony socket containing the eyeball and related structures. All Critical to evaluate in midface trauma for fractures and entrapment. Inferior Orbital Fissure 23 Fissure in the orbital floor transmitting nerves and vessels. Coronal, Axial Landmark in orbital fracture assessment. Infraorbital Canal 24 Canal in the orbital floor for the infraorbital nerve/vessels. Coronal, Sagittal Can protrude into the maxillary sinus; at risk during sinus surgery. Lacrimal Bone 26 Small bone in the medial orbital wall. Coronal, Axial Forms part of the fossa for the lacrimal sac. Nasolacrimal Canal 46 Bony canal draining tears into the nasal cavity. Sagittal, Coronal Relevant in orbital and sinus surgery (e.g., DCR). Cranial Sutures 45, 58 Junctions between cranial bones (e.g., Nasofrontal). All Assessed for fusion in growth analysis and for diastasis in trauma. Soft Tissues & Spaces
Infratemporal Fossa 25 Space medial to the mandibular ramus. Axial, Coronal Site for displaced third molars; pathway for infection/tumors. Pterygopalatine Fossa 54 Small space posterior to the maxilla. Sagittal, Coronal Key junction for neurovascular structures; target for nerve blocks. Nasopharynx/Oropharynx 47/49 Upper portions of the pharyngeal airway. Sagittal Dimensions are critical for assessing obstructive sleep apnea. Parapharyngeal Space 50 Fascial space lateral to the pharynx. Axial, Coronal Site for tumors and deep neck infections. Submandibular Space 60 Fascial space below the floor of the mouth. Axial, Coronal Site of Ludwig's angina, a life-threatening cellulitis. Submandibular Gland 61 Salivary gland in the submandibular space. Axial, Coronal Its fossa can create a deep lingual concavity, a risk for implant surgery. Tongue/Uvula 62/64 Soft tissue structures of the oral cavity/oropharynx. Sagittal Position and size influence airway patency. Mandibular Structures The mandible is a complex U-shaped bone that houses the lower dentition and articulates with the cranium at the temporomandibular joints. Its intricate anatomy contains critical neurovascular structures that must be precisely located prior to any surgical intervention. The mandibular ramus is the vertical portion of the mandible, extending from the angle to the condylar and coronoid processes. It is a structure of immense surgical importance, serving as the primary site for osteotomies in orthognathic surgery, such as the bilateral sagittal split osteotomy (BSSO), and as a common intraoral donor site for autogenous bone grafts. CBCT allows for precise pre-surgical measurement of its buccolingual thickness, which is a critical factor in preventing unfavorable fractures or "bad splits" during BSSO. The coronoid process is a triangular, flat projection from the anterosuperior aspect of the ramus, serving as the insertion point for the temporalis muscle. On sagittal CBCT views, its shape is most commonly triangular but can also appear rounded. Its clinical significance extends to maxillofacial trauma, where it can be fractured, and to reconstructive surgery, where it can be harvested as a donor graft. In rare cases of elongation, it can impinge on the zygomatic arch, limiting mandibular movement. The mandibular condyle is the articulating process of the mandible, forming the movable component of the TMJ. Its morphology is highly variable and can be classified on coronal and sagittal views as convex, round, flat, or angled. A thorough CBCT assessment of condylar morphology, position within the glenoid fossa, and osseous integrity is fundamental for the diagnosis of temporomandibular disorders (TMD) and for planning orthognathic surgery. The mandibular notch is the deep concavity separating the condylar and coronoid processes. It allows passage of the masseteric nerve and vessels. Its shape, typically classified as round or triangular on sagittal views, is dependent on the morphology of the adjacent processes. It serves as an important landmark for determining the height of osteotomies on the ramus. The mandibular canal (also known as the inferior alveolar canal) is a radiolucent channel that traverses the body and ramus of the mandible, housing the inferior alveolar neurovascular bundle. Its visibility on CBCT can vary, with cortical borders appearing well-defined in some individuals and poorly defined in others, and visualization often becomes more difficult in the anterior regions near the mental foramen. Tracing the exact course of this canal is one of the most critical steps in planning for the placement of dental implants or the extraction of impacted third molars to prevent iatrogenic nerve injury. The mandibular foramen is the opening on the medial surface of the ramus where the inferior alveolar nerve enters the mandibular canal. Its precise vertical and anteroposterior location is highly variable, which directly impacts the success rate of inferior alveolar nerve block anesthesia. CBCT provides accurate measurements of its position relative to the occlusal plane and the anterior border of the ramus, aiding in more predictable anesthetic techniques and safer ramus osteotomies. The mental foramen is the anterior exit of the mandibular canal, typically located in the apical region of the mandibular premolars. It appears as a distinct round or oval radiolucency on all CBCT planes. The mental nerve emerges here, providing sensation to the lower lip and chin. A critical anatomical variation is the anterior loop, where the nerve extends mesially beyond the foramen before looping back to exit. Failure to identify this loop on CBCT before placing an implant in the premolar region is a common cause of post-operative neuropathy. The genial tubercles (or mental spines) are bony eminences on the lingual midline of the anterior mandible, serving as attachments for the genioglossus and geniohyoid muscles. Their morphology is highly variable, ranging from the classic four-spine pattern to a single rough eminence or even complete absence. These tubercles are a key landmark in genioglossus advancement surgery for obstructive sleep apnea and must be evaluated when planning implants in the anterior mandible to determine available bone height. The retromolar trigone is the triangular mucosal area posterior to the last mandibular molar. It is an important anatomical site in the staging of oral cancers and a key landmark for prosthodontic considerations related to denture extension. Maxillary, Palatal, and Zygomatic Structures The midface is a complex architectural unit composed of the paired maxillae, palatine, and zygomatic bones, which collectively form the upper jaw, hard palate, cheeks, and the floor of the orbits and nasal cavity. The maxilla is the central bone of the midface, housing the maxillary sinus and the upper dentition. Its evaluation is fundamental to nearly all aspects of dentistry. The maxillary tuberosity, a rounded prominence distal to the third molar, is a primary stress-bearing area crucial for the stability and retention of complete dentures. It is also a site for pterygoid implant placement and orthodontic mini-screw anchorage, particularly when posterior teeth are missing. The hard palate, forming the roof of the mouth, is composed of the palatine processes of the maxilla and the horizontal plates of the palatine bones. The thickness of the palatal bone and its overlying mucosa, which can be precisely measured on coronal and sagittal CBCT views, is a critical determinant for the primary stability of orthodontic miniscrews. The middle suture of the hard palate (midpalatal suture) runs along the midline. The maturational stage of this suture, classified from Stage A (open) to Stage E (fused) on axial CBCT images, is the single most important factor in determining whether maxillary transverse deficiency in an adolescent or young adult can be treated with conventional rapid palatal expansion (RME) or requires surgical assistance (SARPE). The incisive canal (or nasopalatine canal) is a neurovascular conduit in the anterior midline of the maxilla, connecting the oral and nasal cavities. Its shape is highly variable, appearing as cylindrical, funnel-shaped, or hourglass-shaped on sagittal views, and it can have multiple smaller canals. Its oral opening is the incisive foramen. Due to its location, the incisive canal is a major obstacle for implant placement in the maxillary central incisor position. Pre-surgical CBCT assessment is mandatory to measure its diameter and trajectory to avoid encroachment, which can lead to implant failure or sensory disturbances. The greater palatine canal and the more posterior lesser palatine canals transmit the corresponding neurovascular bundles from the pterygopalatine fossa to the hard and soft palate. Identifying the foramina of these canals is essential for administering effective palatal anesthesia and for planning surgical procedures on the palate to avoid neurovascular injury. The anterior nasal spine (ANS) is a midline projection of bone at the inferior margin of the nasal aperture. Its size and angulation, clearly visible on sagittal and coronal CBCT views, influence the esthetic profile of the nasolabial angle and can limit the available bone height for implant placement in the anterior maxilla. The zygoma (cheekbone) and the zygomatic arch form the lateral prominence of the midface. These structures are critical in the assessment of facial trauma, as they are components of zygomaticomaxillary complex (ZMC) fractures. The body of the zygoma also serves as the anchor point for zygomatic implants, an advanced solution for rehabilitating the severely atrophic maxilla. Cranial Base and Sphenoid Complex The cranial base, particularly the sphenoid and temporal bones, contains numerous foramina and processes that are frequently visualized in large FOV CBCT scans. While often considered outside the traditional realm of dentistry, these structures are critical landmarks for advanced surgical procedures and can be the site of significant incidental pathology. The sphenoid bone is a complex, unpaired bone at the base of the skull. Its greater wings form a portion of the middle cranial fossa floor and the lateral orbital walls. Embedded within the greater wings are several critical foramina. The foramen ovale, best visualized on axial and coronal planes, transmits the mandibular division of the trigeminal nerve (CN V3). The foramen rotundum, located anteromedial to the foramen ovale, transmits the maxillary division (CN V2). These foramina are key landmarks in skull base surgery and for diagnosing perineural tumor spread. The pterygoid processes are inferior projections from the sphenoid bone, each dividing into a medial and lateral pterygoid plate. These plates form the posterior boundary of the pterygopalatine fossa and serve as attachment sites for the pterygoid and tensor veli palatini muscles. The integrity of the pterygoid plates is a defining feature in the Le Fort classification of midface fractures and a critical consideration during pterygomaxillary separation in orthognathic surgery. The pterygoid hamulus, a small hook-like extension of the medial plate, can become elongated and cause orofacial pain, a condition known as hamular bursitis. The temporal bone houses the structures of the middle and inner ear. The glenoid (or mandibular) fossa is the concavity that articulates with the mandibular condyle. The carotid canal provides passage for the internal carotid artery; while the canal itself may be at the periphery of a dental CBCT, calcifications within the artery are a critical incidental finding. The styloid process is a slender projection that, if elongated beyond 30 mm, can impinge on cranial nerves or the carotid artery, causing pain, dysphagia, and dizziness—a constellation of symptoms known as Eagle syndrome. The external auditory canal's anterior wall is formed by the tympanic plate of the temporal bone and is in close proximity to the TMJ; posterior displacement of the condyle during trauma can fracture this wall. At the inferior edge of large FOV scans, portions of the cervical spine are often visible. The dens axis, or odontoid process of the second cervical vertebra (C2), is a key landmark. Incidental findings in this region can include fractures from trauma or developmental anomalies like os odontoideum, which can cause significant instability. The hyoid bone, a U-shaped bone suspended in the neck, is an important indicator of tongue posture and airway dimensions, making its position relevant in the assessment of OSA and in planning for orthognathic surgery. Nasal, Sinus, and Orbital Structures The CBCT volume provides an unparalleled view of the intricate anatomy of the nasal cavity, paranasal sinuses, and orbits. The nasal cavity airway is delineated by the nasal bones superiorly, the hard palate inferiorly, and the nasal septum medially. The septum itself is a composite structure formed by the vomer, the perpendicular plate of the ethmoid bone, and anterior cartilage. Deviations of the septum are common and can contribute to airway obstruction. Projecting from the lateral nasal walls are the conchae (turbinates), which create the inferior and middle meatuses—critical drainage pathways for the sinuses and nasolacrimal duct. An important anatomical variant is concha bullosa, the pneumatization of a turbinate (most often the middle), which can narrow the middle meatus and impede sinus drainage. The four paired paranasal sinuses—frontal, ethmoid, maxillary, and sphenoid—are frequently sites of incidental pathology. A systematic review must assess for signs of sinusitis, such as mucosal thickening, polyps, or fluid retention. The maxillary sinus is of particular dental significance due to its proximity to the roots of the posterior maxillary teeth and its role in sinus augmentation procedures for implant placement. The sphenoid sinus is highly variable in its pneumatization and is divided by one or more sphenoid sinus septa. Its close relationship to the optic nerve and internal carotid artery makes it a critical area in endoscopic sinus and transsphenoidal surgery. Superior to the nasal complex are structures of the anterior cranial fossa and orbits. The crista galli is a vertical projection of the ethmoid bone that serves as an attachment for the falx cerebri. The orbit is the bony socket containing the eye. Its floor is also the roof of the maxillary sinus, and its medial wall is the thin lamina papyracea of the ethmoid. These are the weakest points of the orbit and are the common sites for "blowout" fractures in maxillofacial trauma. Neurovascular structures pass through the inferior orbital fissure and the infraorbital canal, which can occasionally protrude into the maxillary sinus, placing the infraorbital nerve at risk during sinus surgery. Tears drain from the eye via the lacrimal bone and into the nasolacrimal canal, which opens into the inferior meatus. This duct can be obstructed, requiring surgical intervention (dacryocystorhinostomy, or DCR). Finally, cranial sutures such as the nasofrontal and sphenozygomatic sutures are important landmarks for assessing growth and diagnosing fracture displacement. Soft Tissues and Fascial Spaces Although CBCT has limited soft tissue contrast, it can delineate the boundaries of fascial spaces and airway passages, which is crucial for assessing the spread of infection, tumor growth, and airway patency. The infratemporal fossa and pterygopalatine fossa are deep anatomical spaces containing muscles of mastication, cranial nerves, and major blood vessels. They are important pathways for administering regional anesthesia but also for the spread of odontogenic infections and tumors. Displaced maxillary third molars can also be lost into these spaces during extraction. The pharyngeal airway is divided into the nasopharynx (posterior to the nasal cavity) and the oropharynx (posterior to the oral cavity). The dimensions and volume of these spaces, readily measured on sagittal CBCT views, are directly related to the risk of obstructive sleep apnea. Soft tissue structures like the tongue and uvula can be visualized, and their size and position contribute to airway patency. The deep fascial spaces of the neck, including the parapharyngeal space and submandibular space, are also partially visible. The submandibular space is the site of Ludwig's angina, a rapidly spreading and life-threatening cellulitis that often originates from an infected mandibular molar. The submandibular gland resides in a fossa on the lingual aspect of the mandible, which can create a deep concavity. Failure to recognize this concavity on a CBCT scan prior to implant placement can lead to lingual cortical plate perforation, a severe surgical complication. Figure Legends for Dental Tomography (Figures 6, 7, and 8) The following legends correspond to the anatomical structures labeled in the figures from the chapter "Diagnostic Imaging in Oral and Maxillofacial Pathology". Figure 6. 3D CT anatomy of the facial skeleton. Figure 7. (A,B,C,D). Axial CT anatomy of the facial skeleton. Figure 8. (A,B,C,D,E,F). Coronal CT anatomy of the facial skeleton. 1. Anterior nasal spine 2. Carotid canal 3. Concha bullosa 4. Coronoid process 5. Crista galli 6. Dens axis 7. Ethmoid sinus 8. External auditory canal 9. Foramen ovale 10. Foramen rotundum 11. Frontal bone 12. Frontal sinus 13. Genial tubercle of mandible 14. Glenoid fossa 15. Greater palatine canal 16. Greater wing of sphenoid bone 17. Hamulus of medial pterygoid plate 18. Hard palate 19. Hyoid bone 20. Incisive canal 21. Incisive foramen 22. Inferior meatus 23. Inferior orbital fissure 24. Infraorbital canal 25. Infratemporal fossa 26. Lacrimal bone 27. Lateral pterygoid plate 28. Lesser palatine canal 29. Mandible 30. Mandibular canal 31. Mandibular condyle 32. Mandibular foramen 33….source alone. Its value is unlocked only through the symbiosis of advanced imaging capabilities with a clinician's deep, three-dimensional understanding of anatomy and a commitment to a rigorous, systematic interpretation protocol. The CBCT scanner provides the raw data; it is the clinician's knowledge and disciplined approach that transform that data into meaningful diagnostic information. The adoption of a systematic, full-volume review forces a cognitive shift, expanding the practitioner's diagnostic purview from the dentoalveolar complex to the entire maxillofacial region. This expanded diagnostic responsibility elevates the role of the dental professional. By identifying incidental findings ranging from sinus pathology and airway compromise to vascular disease and occult fractures, the dentist becomes an integral and vital sentinel in the patient's overall healthcare journey. The integration of comprehensive CBCT analysis into daily practice is therefore not just a matter of technological advancement; it is a commitment to a higher standard of care, enhancing surgical predictability, improving patient safety, and solidifying the dental professional's role as an integrated healthcare provider. Works cited 1. Cone beam computed tomography: basics and applications in …, https://pmc.ncbi.nlm.nih.gov/articles/PMC5750833/ 2. Introduction – Cone-Beam Computed Tomography (CBCT) Applications in Dentistry, https://www.dentalcare.com/en-us/ce-courses/ce531/introduction 3. The Application of Cone Beam Computed Tomography (CBCT) on the Diagnosis and Management of Maxillofacial Trauma – MDPI, https://www.mdpi.com/2075-4418/14/4/373 4. CBCT anatomical structures | PPTX – Slideshare, https://www.slideshare.net/slideshow/cbct-anatomical-structures/261685800 5. CBCT for Diagnostics, Treatment Planning and Monitoring of Sinus Floor Elevation Procedures – MDPI, https://www.mdpi.com/2075-4418/13/10/1684 6. The anterior nasal spine is seen on cross-sectional view – ResearchGate, https://www.researchgate.net/figure/The-anterior-nasal-spine-is-seen-on-cross-sectional-view_fig4_287537512 7. Dental Cone Beam CT – Radiologyinfo.org, https://www.radiologyinfo.org/en/info/dentalconect 8. Cone-Beam Computed Tomography for Oral and Maxillofacial Imaging – ResearchGate, https://www.researchgate.net/publication/319139714_Cone-Beam_Computed_Tomography_for_Oral_and_Maxillofacial_Imaging 9. Systematic interpretation of CBCT scans: why do it? | Request PDF – ResearchGate, https://www.researchgate.net/publication/260808004_Systematic_interpretation_of_CBCT_scans_why_do_it 10. Cone Beam CT Interpretation – American Association of Endodontists, https://www.aae.org/specialty/cone-beam-ct-interpretation/ 11. CBCT Dental Applications – Capture 3D Radiology, https://www.capture3dr.com/education/cbct-dental-applications/ 12. Guide to Interpreting CBCT Scans in Endodontics – 3Beam | Cutting …, https://3beam.co.uk/guide-to-interpreting-cbct-scans-in-endodontics/ 13. 9: How to Interpret Cone Beam Computed Tomography Scans | Pocket Dentistry, https://pocketdentistry.com/9-how-to-interpret-cone-beam-computed-tomography-scans/ 14. Patterns of Cone-Beam Computed Tomography (CBCT) Utilization by Various Dental Specialties: A 4-Year Retrospective Analysis from a Dental and Maxillofacial Specialty Center – MDPI, https://www.mdpi.com/2227-9032/9/8/1042 15. CBCT interpretation for dental implant treatment planning, https://www.creighton.edu/sites/default/files/2022-10/3%20Paneer.pdf 16. Step-by-Step Guide to the CBCT Scan Process for Dental Imaging – Odonto Dental, https://www.odontodental.ca/blog/a-step-by-step-guide-to-the-cbct-scan-process/ 17. Image Interpretation – Cone-Beam Computed Tomography (CBCT) Applications in Dentistry, https://www.dentalcare.com/en-us/ce-courses/ce531/image-interpretation 18. Mastering CBCT: Essential Fundamentals for Successful 3D Dental Radiography, https://www.dentalti.com/post/mastering-cbct-essential-fundamentals-for-successful-3d-dental-radiography 19. Understanding Normal Anatomy on Dental CBCT Scans – Ct-dent.co.uk, https://ct-dent.co.uk/understanding-normal-anatomy-on-dental-cbct-scans/ 20. How a Cone Beam CT Saved a Dental Patient's Life – Spear Education, https://www.speareducation.com/spear-review/2015/09/pay-attention-save-a-life 21. Evaluation of maxillary sinus in health and disease through CBCT …, https://ijohd.org/archive/volume/10/issue/3/article/12390 22. (PDF) Hidden Pathologies of Maxillary Sinus using CBCT Scans – ResearchGate, https://www.researchgate.net/publication/355290427_Hidden_pathologies_of_maxillary_sinus_using_CBCT_scans 23. Mandibular ramus thickness based on cone beam computed tomography scan, https://www.researchgate.net/publication/327494232_Mandibular_ramus_thickness_based_on_cone_beam_computed_tomography_scan 24. Determination of the Volume and Density of Mandibular Ramus as a …, https://pmc.ncbi.nlm.nih.gov/articles/PMC9989044/ 25. A STUDY OF MANDIBULAR ANATOMY FOR ORTHOGNATHIC SURGERY IN KOREANS, https://www.jkaoms.org/journal/view.html?volume=28&number=2&page=126 26. (PDF) Evaluation of mandibular notch, coronoid process, and …, https://www.researchgate.net/publication/320719919_Evaluation_of_mandibular_notch_coronoid_process_and_mandibular_condyle_configurations_with_cone_beam_computed_tomography 27. Evaluation of mandibular notch, coronoid process, and mandibular condyle configurations with cone beam computed tomography | Abstract – Allied Academies, https://www.alliedacademies.org/abstract/evaluation-of-mandibular-notch-coronoid-process-and-mandibular-condyle-configurations-with-cone-beam-computed-tomography-8613.html 28. A study on coronoid process of the dry adult human mandibles – ResearchGate, https://www.researchgate.net/publication/305951934_A_study_on_coronoid_process_of_the_dry_adult_human_mandibles 29. Conservative Management of the Isolated Mandibular Coronoid Process Fracture, https://bezmialemscience.org/articles/conservative-management-of-the-isolated-mandibular-coronoid-process-fracture/bas.galenos.2019.2926 30. A 3D cone beam computed tomography (CBCT) investigation of …, https://pmc.ncbi.nlm.nih.gov/articles/PMC8589592/ 31. CBCT image showing the condyle measurement in the coronal view – ResearchGate, https://www.researchgate.net/figure/CBCT-image-showing-the-condyle-measurement-in-the-coronal-view-the-condylar-height-and_fig8_308182010 32. Morphometric analysis of mandibular notch in dry human mandibles- A surgeon's guide to the masseteric nerve block – Cumhuriyet Dental Journal, http://cdj.cumhuriyet.edu.tr/en/pub/issue/69076/987053 33. Visibility of the mandibular canal on CBCT cross-sectional images …, https://pmc.ncbi.nlm.nih.gov/articles/PMC4234336/ 34. Mandibular canal location: Cone-beam computed tomography examination, https://experts.umn.edu/en/publications/mandibular-canal-location-cone-beam-computed-tomography-examinati 35. Journal of Oral Implantology, https://joi.kglmeridian.com/page/implant-placement-in-the-posterior-mandible-is-important-to-avoid-injury-to-the-ian 36. Assessing the Mandibular Foramen: A Cone Beam Computed …, https://opendentistryjournal.com/VOLUME/19/ELOCATOR/e18742106396893/FULLTEXT/ 37. (PDF) Mandibular foramen location – ResearchGate, https://www.researchgate.net/publication/337003376_Mandibular_foramen_location 38. (PDF) Cone Beam CT Description of Mental Foramen Variants: A …, https://www.researchgate.net/publication/381893922_Cone_Beam_CT_Description_of_Mental_Foramen_Variants_A_Review 39. Topography of mental foramen in a selected Belarusian population according to cone beam computed tomography – Open Access Journals, https://www.openaccessjournals.com/articles/topography-of-mental-foramen-ina-selected-belarusian-populationaccording-to-cone-beam-computedtomography.html 40. Clinical and Surgical Relevance of Mental Foramen Variations in Mandibular Anatomy – A Morphometric Insight | European Journal of Cardiovascular Medicine, https://healthcare-bulletin.co.uk/article/clinical-and-surgical-relevance-of-mental-foramen-variations-in-mandibular-anatomy-a-morphometric-insight-4323/ 41. Assessment of the Anterior Loop and Pattern of Entry of Mental Nerve Into the Mental Foramen: A Radiographic Study of Panoramic Images – PMC, https://pmc.ncbi.nlm.nih.gov/articles/PMC10995115/ 42. Assessment of Genial Tubercle with CBCT with Clinical Relevance, https://ijmi.in/archive/volume/3/issue/2/article/6320/pdf 43. Genial tubercles: Morphological study of the controversial …, https://pmc.ncbi.nlm.nih.gov/articles/PMC6682497/ 44. Analysis of Genial Tubercle Anatomy Using Cone Beam Computed Tomography – A Retrospective Study from Chennai, India – ResearchGate, https://www.researchgate.net/publication/354953173_Analysis_of_Genial_Tubercle_Anatomy_Using_Cone_Beam_Computed_Tomography_-_A_Retrospective_Study_from_Chennai_India 45. Definition of retromolar trigone – NCI Dictionary of Cancer Terms – NCI, https://www.cancer.gov/publications/dictionaries/cancer-terms/def/retromolar-trigone 46. Techniques, Tricks, and Stratagems of Oral Cavity Computed Tomography and Magnetic Resonance Imaging – MDPI, https://www.mdpi.com/2076-3417/12/3/1473 47. CBCT/3-D Imaging | Dental School – Boston University, https://www.bu.edu/dental/patient-care/patient-guide/services/cbct-3d/ 48. CBCT Cyst Leasions Diagnosis Imaging Mandible Maxilla – PMC, https://pmc.ncbi.nlm.nih.gov/articles/PMC4064885/ 49. (PDF) Cone-Beam Computed Tomographic Evaluation of Maxillary …, https://www.researchgate.net/publication/343818922_Cone-Beam_Computed_Tomographic_Evaluation_of_Maxillary_Tuberosity_after_the_Extraction_of_Maxillary_Third_Molars 50. Anatomical Landmarks of Maxilla: Essential Guide for Dental Pros – Implant League, https://implantleaguecourses.com/anatomical-landmarks-of-maxilla-essential-guide-for-dental-pros/ 51. Axial CBCT slice through the maxillary tuberosities. (1) maxillary… | Download Scientific Diagram – ResearchGate, https://www.researchgate.net/figure/Axial-CBCT-slice-through-the-maxillary-tuberosities-1-maxillary-sinus-2_fig10_388279472 52. -Occlusal view of a palate in CBCT. The horizontal lines represent …, https://www.researchgate.net/figure/Occlusal-view-of-a-palate-in-CBCT-The-horizontal-lines-represent-the-sites-of-coronal_fig1_221841839 53. A Retrospective Investigation of the Hard Palate Morphometry with 416 Cone-Beam CT Images, https://www.academicmed.org/Uploads/Volume4Issue2/6.-57576-25-29.pdf 54. HOW to measure CBCT BEFORE AND AFTER MID PALATAL SUTURE OPENING | PPTX, https://www.slideshare.net/slideshow/how-to-measure-cbct-before-and-after-mid-palatal-suture-opening/68924980 55. Morphological Analysis of Stages of Midpalatal Suture Maturation in …, https://intjmorphol.com/wp-content/uploads/2025/04/Art_30_432_2025.pdf 56. Midpalatal Suture Maturation in Relation to Age, Sex, and Facial Skeletal Growth Patterns: A CBCT Study – PubMed Central, https://pmc.ncbi.nlm.nih.gov/articles/PMC11353169/ 57. Cone Beam Computed Tomography Assessment of the Maxillary …, https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0117251 58. Incisive canal: Variations on cone beam computed tomography and its impact on dental implant planning – IP Annals of Prosthodontics and Restorative Dentistry, https://aprd.in/html-article/16078 59. Measurement of incisive foramen (blue line), nasal foramen (red line),… – ResearchGate, https://www.researchgate.net/figure/Measurement-of-incisive-foramen-blue-line-nasal-foramen-red-line-incisive-diameter_fig5_273953195 60. Evaluation of the incisive canal using cone beam computed tomography – Redalyc, https://www.redalyc.org/journal/6100/610075182005/html/ 61. The Incisive Canal: A Comprehensive Review – ResearchGate, https://www.researchgate.net/publication/326705914_The_Incisive_Canal_A_Comprehensive_Review 62. Radiomorphometric analysis of the Greater Palatine Canal and the …, https://www.dovepress.com/radiomorphometric-analysis-of-the-greater-palatine-canal-and-the-ptery-peer-reviewed-fulltext-article-CCIDE 63. Cone Beam Computed Tomographic Analysis of Anatomical Variations of Greater Palatine Canal and Foramen in Relation to Gender in South Indian Population – Walsh Medical Media, https://www.walshmedicalmedia.com/open-access/cone-beam-computed-tomographic-analysis-of-anatomical-variations-of-greater-palatine-canal-and-foramen-in-relation-to-gender-in-south-indian-population-2247-2452-1000844.pdf 64. Anatomy of the greater palatine foramen and canal and their clinical significance in relation to the greater palatine artery: a systematic review and meta-analysis – PubMed, https://pubmed.ncbi.nlm.nih.gov/36640185/ 65. Lesser palatine nerves | Radiology Reference Article | Radiopaedia …, https://radiopaedia.org/articles/lesser-palatine-nerves 66. Radiographic and clinical evaluation of anterior nasal spine …, https://www.bioinformation.net/021/973206300212820.pdf 67. Anatomical Description of anterior nasal spine | Download Scientific Diagram – ResearchGate, https://www.researchgate.net/figure/Anatomical-Description-of-anterior-nasal-spine_fig7_344136214 68. Nasal–upper lip complex – Pocket Dentistry, https://pocketdentistry.com/nasal-upper-lip-complex/ 69. Evaluation of the zygomatic bone prior to the quad zygoma surgery …, https://pmc.ncbi.nlm.nih.gov/articles/PMC12482155/ 70. Evaluation of the zygomatic bone by cone beam computed tomography – ResearchGate, https://www.researchgate.net/publication/263296725_Evaluation_of_the_zygomatic_bone_by_cone_beam_computed_tomography 71. Cone beam computed tomography evaluation of sphenoid sinus in different sagittal skeletal pattern – PMC, https://pmc.ncbi.nlm.nih.gov/articles/PMC9826704/ 72. Anatomy and Diseases of the Greater Wings of the Sphenoid Bone – RSNA Journals, https://pubs.rsna.org/doi/full/10.1148/rg.210094 73. Foramen ovale (skull) | Radiology Reference Article | Radiopaedia.org, https://radiopaedia.org/articles/foramen-ovale-skull 74. Foramen rotundum | Radiology Reference Article | Radiopaedia.org, https://radiopaedia.org/articles/foramen-rotundum 75. (PDF) Extraoral anatomy in CBCT – a literature review. Part 3: Retromaxillary region, https://www.researchgate.net/publication/339913634_Extraoral_anatomy_in_CBCT_-_a_literature_review_Part_3_Retromaxillary_region 76. Pterygoid processes | Radiology Reference Article | Radiopaedia.org, https://radiopaedia.org/articles/pterygoid-processes 77. Pterygoid process – e-Anatomy – IMAIOS, https://www.imaios.com/en/e-anatomy/anatomical-structures/pterygoid-process-1536896660 78. CBCT-Based measurement of lateral pterygoid muscle length in TMJ dysfunction – PubMed, https://pubmed.ncbi.nlm.nih.gov/41013438/ 79. Medial pterygoid plate – e-Anatomy – IMAIOS, https://www.imaios.com/en/e-anatomy/anatomical-structures/medial-pterygoid-plate-1536896692 80. Anatomy, Head and Neck, Medial Pterygoid Muscle – StatPearls – NCBI, https://www.ncbi.nlm.nih.gov/books/NBK546588/ 81. Radiological examination of the relationship between the pterygomaxillary junction and fracture pattern – JournalAgent, https://jag.journalagent.com/z4/download_fulltext.asp?pdir=travma&plng=tur&un=UTD-45995 82. Cone beam computed tomography axial view showing an elongated pterygoid hamulus. – ResearchGate, https://www.researchgate.net/figure/Cone-beam-computed-tomography-axial-view-showing-an-elongated-pterygoid-hamulus_fig4_326993450 83. Investigating the Morphologic Indices of the Hamulus Pterygoid …, https://www.jrmds.in/articles/investigating-the-morphologic-indices-of-the-hamulus-pterygoid-process-using-the-cbct-technique.pdf 84. Assessment of Condyle and Glenoid Fossa Morphology Using …, https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0121682 85. Improved Visualization and Assessment of Condylar Position in the Glenoid Fossa for Different Occlusions: A CBCT Study – The Journal of Contemporary Dental Practice, https://thejcdp.com/doi/JCDP/pdf/10.5005/jp-journals-10024-1912 86. Carotid canal – e-Anatomy – IMAIOS, https://www.imaios.com/en/e-anatomy/anatomical-structures/carotid-canal-1536895848 87. Cone beam computed tomographic evaluation of styloid process: A …, https://pmc.ncbi.nlm.nih.gov/articles/PMC5502567/ 88. Fractured styloid process masquerading as neck pain – KoreaMed Synapse, https://synapse.koreamed.org/articles/1089169 89. Eagle Syndrome – StatPearls – NCBI Bookshelf, https://www.ncbi.nlm.nih.gov/books/NBK430789/ 90. Foramen of Huschke in the External Auditory Canal Misattributed to Temporomandibular Disorders: Case Reports – Journal of Oral Medicine and Pain, https://www.journalomp.org/journal/view.html?doi=10.14476/jomp.2025.50.1.34 91. Imaging of external auditory canal fractures associated … – DergiPark, https://dergipark.org.tr/tr/download/article-file/846934 92. Anatomy of the teeth: annotated dental-CBCT – IMAIOS, https://www.imaios.com/en/e-anatomy/head-and-neck/dental-cbct 93. The Dens: Normal Development, Developmental Variants and …, https://clinicalimagingscience.org/the-dens-normal-development-developmental-variants-and-anomalies-and-traumatic-injuries/ 94. Axis (C2) | Radiology Reference Article | Radiopaedia.org, https://radiopaedia.org/articles/axis-c2 95. A CBCT Morphometric Study of Hyoid Bone According to Skeletal …, https://www.mdpi.com/2227-9032/13/19/2423 96. A CBCT Morphometric Study of Hyoid Bone According to Skeletal and Breathing Patterns Using Multi-Factor Robust ANOVA – Preprints.org, https://www.preprints.org/frontend/manuscript/10095792e5d7134cfbd8e125845c7851/download_pub 97. oral surgeon Allentown PA – What is Hyoid Advancement Surgery, https://lehighoms.com/p/BLOG-107748-2023.9.25-What-is-Hyoid-Advancement-Surgery-p.asp?fc=1 98. Anatomy, Head and Neck, Ethmoid Bone – StatPearls – NCBI …, https://www.ncbi.nlm.nih.gov/books/NBK544328/ 99. (PDF) Congenital Vomer Agenesis: A Rare and Poorly Understood …, https://www.researchgate.net/publication/323138311_Congenital_Vomer_Agenesis_A_Rare_and_Poorly_Understood_Condition_Revealed_by_Cone_Beam_CT 100. Nasal Septal Deviation and Nasofacial Skeletal Form – University Digital Conservancy, https://conservancy.umn.edu/bitstreams/4c08e143-1f35-49bb-8958-1ef6805f782f/download 101. The nasal septum deviation index (NSDI) based on CBCT data, https://pubmed.ncbi.nlm.nih.gov/26783044/ 102. Anatomy, Head and Neck, Nose Paranasal Sinuses – StatPearls – NCBI Bookshelf, https://www.ncbi.nlm.nih.gov/books/NBK499826/ 103. Cone Beam Computed Tomography for the Nasal Cavity and …, https://pocketdentistry.com/cone-beam-computed-tomography-for-the-nasal-cavity-and-paranasal-sinuses/ 104. The Prevalence of Concha Bullosa and Nasal Septal Deviation and …, https://pmc.ncbi.nlm.nih.gov/articles/PMC2938434/ 105. Incidental finding of bullous concha by cone beam computed tomography – SciELO, https://www.scielo.sa.cr/scielo.php?script=sci_arttext&pid=S2215-34112022000100026 106. MAXILLARY SINUS IMPLICATIONS IN ENDODONTICS AND IMPLANT DENTISTRY – A LITERATURE REVIEW – Romanian Journal of Oral Rehabilitation, http://rjor.ro/wp-content/uploads/2024/06/MAXILLARY-SINUS-IMPLICATIONS-IN-ENDODONTICS.pdf 107. Maxillary Sinus Augmentation – Pocket Dentistry, https://pocketdentistry.com/maxillary-sinus-augmentation/ 108. Cone Beam Computed Tomography Analysis of Sphenoid Sinus …, https://pmc.ncbi.nlm.nih.gov/articles/PMC7855127/ 109. Computed tomographic study of sphenoid sinus and its septations, https://ijcap.org/archive/volume/6/issue/3/article/22665 110. What is Transsphenoidal Surgery? | Pituitary Center – Barrow Neurological Institute, https://www.barrowneuro.org/treatment/transsphenoidal-surgery/ 111. Crista galli – e-Anatomy – IMAIOS, https://www.imaios.com/en/e-anatomy/anatomical-structures/crista-galli-129904 112. Crista galli | Radiology Reference Article | Radiopaedia.org, https://radiopaedia.org/articles/crista-galli 113. CT & CBCT imaging: assessment of the orbits | Request PDF, https://www.researchgate.net/publication/230861883_CT_CBCT_imaging_assessment_of_the_orbits 114. Orbital Trauma – PMC – PubMed Central, https://pmc.ncbi.nlm.nih.gov/articles/PMC6486387/ 115. Inferior orbital fissure – e-Anatomy – IMAIOS, https://www.imaios.com/en/e-anatomy/anatomical-structures/inferior-orbital-fissure-123884 116. Radiographic Evaluation of Infraorbital Canal Protrusion into … – JOMR, https://www.ejomr.org/JOMR/archives/2020/4/e5/v11n4e5ht.htm 117. CBCT-DCG sagittal image sectioning the lacrimal duct. The figure shows… | Download Scientific Diagram – ResearchGate, https://www.researchgate.net/figure/CBCT-DCG-sagittal-image-sectioning-the-lacrimal-duct-The-figure-shows-a_fig3_361485108 118. Morphometric Evaluation of Nasolacrimal Canal Diameters Using …, https://www.researchgate.net/publication/331844496_Morphometric_Evaluation_of_Nasolacrimal_Canal_Diameters_Using_CBCT_A_Cross-Sectional_Study 119. Dacryocystorhinostomy (DCR) – Ophthalmic Consultants of Vermont, https://ocvermont.com/tear-duct-surgery/dacryocystorhinostomy-dcr/ 120. Coronal CBCT sections: A, Frontonasal suture; B, Frontomaxillary …, https://www.researchgate.net/figure/Coronal-CBCT-sections-A-Frontonasal-suture-B-Frontomaxillary-suture-C_fig2_368309024 121. Sphenozygomatic suture | Radiology Reference Article …, https://radiopaedia.org/articles/sphenozygomatic-suture 122. Orbital Fracture: Significance of lateral wall – PMC, https://pmc.ncbi.nlm.nih.gov/articles/PMC3729708/ 123. Development of a 3D Learning Resource of the Pterygopalatine Fossa Using Cone Beam Computed Tomography For Dental Students – Creighton University, https://researchworks.creighton.edu/esploro/outputs/graduate/Development-of-a-3D-Learning-Resource/991005932525402656 124. The three-dimensional cone beam computed tomography …, https://www.researchgate.net/figure/The-three-dimensional-cone-beam-computed-tomography-reconstruction_fig2_306119172 125. Pterygopalatine fossa – e-Anatomy – IMAIOS, https://www.imaios.com/en/e-anatomy/anatomical-structures/pterygopalatine-fossa-122988 126. (A) Nasopharynx and (B) oropharynx delimitation. | Download …, https://www.researchgate.net/figure/A-Nasopharynx-and-B-oropharynx-delimitation_fig6_51722060 127. Assessment of the Oropharyngeal Space Using CBCT and Its Impact on Volume of Airway Prior and after Denture Placement – The Journal of Contemporary Dental Practice, https://www.thejcdp.com/doi/JCDP/pdf/10.5005/jp-journals-10024-3732 128. Oropharyngeal Collapse Predicts Treatment Response With Oral Appliance Therapy in Obstructive Sleep Apnea, https://academic.oup.com/sleep/article-pdf/29/5/666/8502965/sleep-29-5-666.pdf 129. Airway – White Birch Dental, https://www.whitebirchdental.com/airway 130. Evaluation of tongue volume and oral cavity capacity using cone …, https://pmc.ncbi.nlm.nih.gov/articles/PMC5996000/ 131. Role of CBCT in sleep apnea – A review – IP Int J Maxillofac Imaging, https://ijmi.in/article-details/19283 132. Ludwig angina | Radiology Reference Article | Radiopaedia.org, https://radiopaedia.org/articles/ludwig-angina 133. Submandibular Gland Fossa Assessment with Cone Beam …, https://www.ijss-sn.com/uploads/2/0/1/5/20153321/09_ijss_july_oa09_-_2019.pdf 134. Evaluation of submandibular gland and submandibular … – DergiPark, https://dergipark.org.tr/tr/download/article-file/2397571 135. Assessment of the role of cone beam computed sialography in diagnosing salivary gland lesions – PMC, https://pmc.ncbi.nlm.nih.gov/articles/PMC3604366/ 136. (PDF) Diagnostic Imaging in Oral and Maxillofacial Pathology, https://www.researchgate.net/publication/221921527_Diagnostic_Imaging_in_Oral_and_Maxillofacial_Pathology

